Pulmonary rales, also known as crackles, are abnormal lung sounds that occur during inhalation and are often indicative of underlying respiratory conditions. These sounds are characterized by brief, discontinuous, bubbling or rattling noises, resembling the sound of salt and pepper being poured onto a hard surface. Rales typically arise from the movement of air through airways filled with fluid, mucus, or other secretions, commonly associated with conditions such as pneumonia, heart failure, or chronic obstructive pulmonary disease (COPD). Understanding how pulmonary rales sound is crucial for healthcare professionals, as their presence, intensity, and location can provide valuable insights into the nature and severity of a patient's respiratory issue, guiding diagnosis and treatment decisions.


What You'll Learn
- Crackles vs. Wheezes: Differentiating between crackles (rales) and wheezes based on sound characteristics
- Fine vs. Coarse Rales: Distinguishing fine, high-pitched from coarse, low-pitched rales in auscultation
- Location of Rales: Identifying rales in lung zones (upper, mid, lower) and their significance
- Causes of Rales: Common conditions like pneumonia, heart failure, or pulmonary edema causing rales
- Timing of Rales: Assessing inspiratory vs. expiratory rales and their clinical implications
![]()
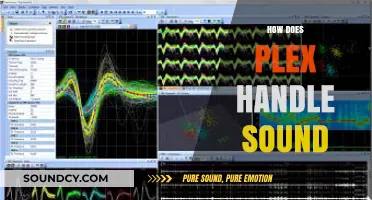
Crackles vs. Wheezes: Differentiating between crackles (rales) and wheezes based on sound characteristics
When auscultating the lungs, it's crucial to differentiate between crackles (also known as rales) and wheezes, as they indicate distinct underlying pathologies. Crackles are characterized by brief, discontinuous, and popping sounds that resemble the noise of opening a velcro strap or crumpling cellophane. They are typically heard during inspiration and can be further classified as fine or coarse. Fine crackles are high-pitched, short, and subtle, often associated with conditions like pulmonary fibrosis or congestive heart failure. Coarse crackles, on the other hand, are louder, lower-pitched, and more easily audible, commonly linked to conditions such as pneumonia or acute bronchitis. Crackles occur due to the sudden popping open of collapsed airways or the movement of air through fluid-filled alveoli.
Wheezes, in contrast, are high-pitched, continuous, and musical sounds that resemble whistling. They are typically heard during both inspiration and expiration, though they may be more prominent during one phase depending on the location and severity of the airway obstruction. Wheezes are caused by the narrowing of airways, often due to conditions like asthma, chronic obstructive pulmonary disease (COPD), or bronchitis. Unlike crackles, wheezes have a sustained quality and can vary in pitch and intensity based on the degree of airway constriction. Wheezes are a hallmark of obstructive lung diseases, where airflow is impeded by inflammation, mucus, or bronchospasm.
One key difference in sound characteristics is the timing of these adventitious lung sounds. Crackles are predominantly inspiratory, as the airflow during inhalation helps to pull open the collapsed or fluid-filled airways. Wheezes, however, can be heard during both inspiration and expiration, with expiratory wheezes being more common in obstructive conditions due to the increased effort required to expel air through narrowed airways. This distinction in timing is a critical clue for clinicians when diagnosing the underlying cause of the abnormal lung sounds.
Another differentiating factor is the quality of the sounds. Crackles are discontinuous and popping, often described as "crackling" or "rattling," whereas wheezes are continuous and musical, with a clear whistling tone. The pitch of crackles tends to be lower in coarse crackles and higher in fine crackles, while wheezes are consistently high-pitched. Additionally, crackles are often localized to specific areas of the lung, whereas wheezes may be more widespread, depending on the extent of airway obstruction.
In practice, differentiating between crackles and wheezes requires careful auscultation and attention to these sound characteristics. Clinicians should note the timing, pitch, continuity, and location of the sounds. For example, a patient with heart failure may present with fine inspiratory crackles at the lung bases, while an asthmatic patient may exhibit widespread expiratory wheezes. Understanding these distinctions is essential for accurate diagnosis and appropriate management of respiratory conditions.
Lastly, it's important to recognize that crackles and wheezes can sometimes coexist in certain conditions, such as severe asthma with concurrent pulmonary edema. In such cases, a thorough clinical assessment, including patient history, physical examination, and additional diagnostic tests, may be necessary to identify the underlying causes and guide treatment. Mastery of auscultation skills and familiarity with these sound characteristics are invaluable tools for healthcare providers in evaluating pulmonary health.
What Does a Pigeon Sound Like? Exploring Their Unique Coos and Calls
You may want to see also
![]()
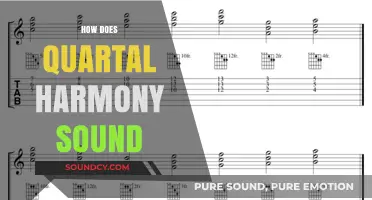
Fine vs. Coarse Rales: Distinguishing fine, high-pitched from coarse, low-pitched rales in auscultation
Pulmonary rales are abnormal breath sounds that can provide crucial insights into a patient's respiratory health. When auscultating the lungs, distinguishing between fine and coarse rales is essential for accurate diagnosis. Fine rales, also known as crackles, are high-pitched and brief, often described as sounding like opening a Velcro strap or crumpling a piece of paper. They are typically heard during inspiration and are more prominent at the end of the inspiratory phase. Fine rales are usually associated with conditions such as pneumonia, acute bronchitis, or pulmonary fibrosis, where fluid or inflammation fills the small airways or alveoli. These sounds are best heard with the stethoscope placed lightly on the chest, as excessive pressure can alter the sound characteristics.
In contrast, coarse rales are low-pitched and bubbling, resembling the sound of air passing through a fluid-filled tube. They are often continuous throughout inspiration and may extend into early expiration. Coarse rales are commonly associated with conditions like chronic bronchitis, bronchiectasis, or congestive heart failure, where there is significant mucus or fluid accumulation in the larger airways. Unlike fine rales, coarse rales are more easily audible and may require less precision in stethoscope placement. The bubbling quality of coarse rales is due to the movement of air through thicker secretions or fluid in the airways, creating a more pronounced and lower-pitched sound.
Distinguishing between fine and coarse rales requires careful attention to pitch, duration, and timing. Fine rales are higher in pitch and shorter in duration, often described as "musical" or "popcorn-like," whereas coarse rales are lower in pitch and longer in duration, with a more "gurgling" or "rattling" quality. The timing of the sounds is also critical: fine rales are predominantly inspiratory, while coarse rales may persist throughout inspiration and into early expiration. Practicing auscultation and familiarizing oneself with these auditory differences is key to mastering the distinction between the two types of rales.
Another important factor in differentiating fine from coarse rales is the patient's clinical context. Fine rales are often associated with acute or inflammatory conditions affecting the distal airways or alveoli, such as pneumonia or acute respiratory distress syndrome (ARDS). Coarse rales, on the other hand, are more commonly linked to chronic conditions involving mucus retention or airway obstruction, like chronic obstructive pulmonary disease (COPD) or cystic fibrosis. Understanding the underlying pathology can help clinicians correlate auscultatory findings with the patient's history and other diagnostic data.
In summary, distinguishing between fine and coarse rales during auscultation involves assessing pitch, duration, timing, and clinical context. Fine rales are high-pitched, brief, and inspiratory, often indicating inflammation or fluid in the small airways or alveoli. Coarse rales are low-pitched, bubbling, and continuous, typically suggesting mucus or fluid in the larger airways. Mastery of these distinctions requires practice and a systematic approach to auscultation, enabling clinicians to accurately identify and address the underlying respiratory conditions.
Does Sound Matter in Writing? Exploring the Power of Auditory Imagery
You may want to see also
![]()
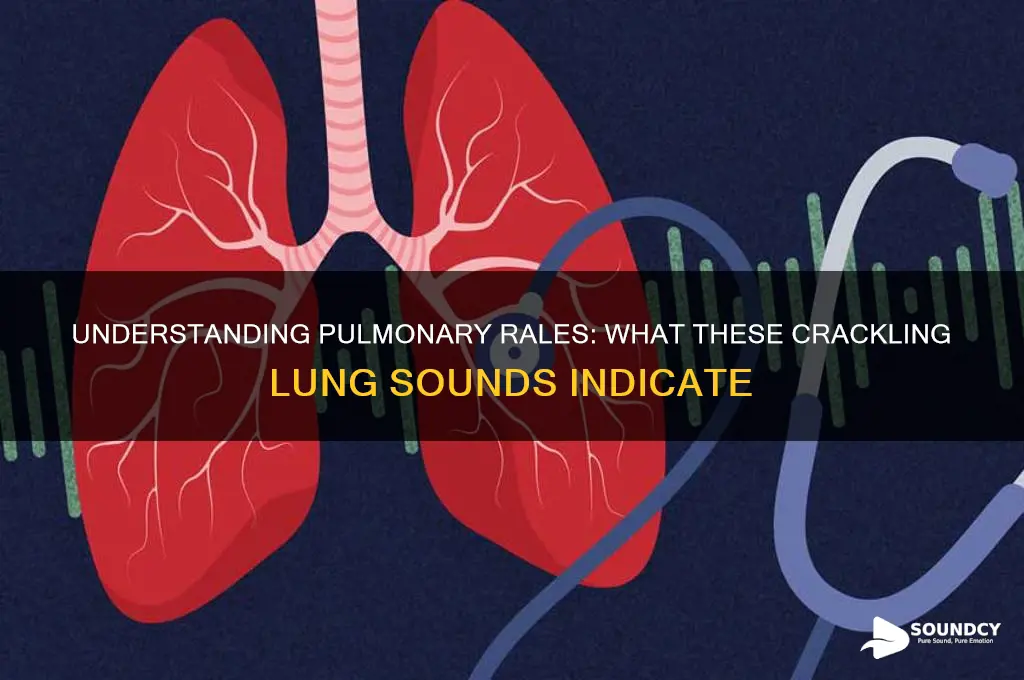
Location of Rales: Identifying rales in lung zones (upper, mid, lower) and their significance
Pulmonary rales, often described as crackling or bubbling sounds during auscultation, are important clinical indicators of underlying lung conditions. The location of these rales—whether in the upper, mid, or lower lung zones—provides valuable insights into the nature and severity of the pathology. Identifying the specific zone where rales are heard can help differentiate between various respiratory disorders, such as pneumonia, heart failure, or interstitial lung disease. For instance, rales in the lower lung zones are commonly associated with conditions like congestive heart failure, where fluid accumulates in the lungs due to poor cardiac function. In contrast, rales in the upper lung zones may suggest conditions like tuberculosis or chronic obstructive pulmonary disease (COPD), depending on other clinical findings.
The upper lung zones, which include the apices and upper lobes, are often auscultated by placing the stethoscope on the shoulders or upper back. Rales in this area can be indicative of infections or inflammatory processes that affect the upper airways. For example, patients with pneumonia or tuberculosis may exhibit coarse, crackling sounds in the upper zones due to the presence of consolidations or infiltrates. Additionally, conditions like sarcoidosis, which causes granulomatous inflammation, may also produce rales in these regions. Recognizing rales in the upper zones prompts further investigation into infectious or inflammatory causes, often requiring imaging studies like chest X-rays or CT scans for confirmation.
The mid-lung zones, located between the upper and lower zones, are assessed by auscultating the chest at the level of the nipples or just below. Rales in this area are less common but can still provide important diagnostic clues. They may indicate conditions such as interstitial lung disease, where fibrosis or scarring affects the lung parenchyma. Patients with conditions like idiopathic pulmonary fibrosis often exhibit fine, velcro-like crackles in the mid-lung zones due to the stiffening of lung tissue. Recognizing rales in this region often necessitates a thorough evaluation of occupational or environmental exposures, as well as advanced imaging and pulmonary function tests to assess lung mechanics.
The lower lung zones, encompassing the lung bases, are auscultated by placing the stethoscope on the front or back of the chest at the level of the sixth to eighth ribs. Rales in these areas are highly suggestive of fluid accumulation, as seen in congestive heart failure or nephrotic syndrome. In heart failure, the backup of blood in the pulmonary circulation leads to pulmonary edema, producing fine or coarse crackles that are often more pronounced during inspiration. Similarly, conditions like pneumonia or aspiration may also cause rales in the lower zones, especially if the infection involves the lung bases. Identifying rales in this region often prompts an evaluation of cardiac function, including echocardiography or BNP levels, to assess for heart failure.
Understanding the significance of rales in different lung zones is crucial for accurate diagnosis and management. For example, bilateral lower zone rales in a patient with paroxysmal nocturnal dyspnea and elevated jugular venous pressure strongly suggest acute heart failure. Conversely, unilateral upper zone rales in a patient with a history of smoking may raise suspicion for lung cancer or chronic infection. Clinicians must correlate auscultatory findings with patient history, physical examination, and diagnostic tests to determine the underlying cause of rales. By systematically assessing the location and characteristics of rales, healthcare providers can tailor their approach to treatment, whether it involves diuresis for heart failure, antibiotics for pneumonia, or corticosteroids for interstitial lung disease.
Unveiling the Sonic Secrets: How Alkhaizer Crafts Unique Sounds
You may want to see also
![]()
Causes of Rales: Common conditions like pneumonia, heart failure, or pulmonary edema causing rales
Pulmonary rales, often described as crackling or bubbling sounds during auscultation, are indicative of underlying respiratory or cardiac conditions. One of the most common causes of rales is pneumonia, an infection that inflames the air sacs in one or both lungs. When pneumonia occurs, the alveoli fill with fluid, pus, or other inflammatory substances, leading to the characteristic crackling sounds heard during inhalation. These rales are typically localized to the affected area of the lung and may be accompanied by symptoms like cough, fever, and shortness of breath. Pneumonia can be caused by bacteria, viruses, or fungi, and its severity ranges from mild to life-threatening, depending on the causative agent and the patient’s overall health.
Heart failure is another frequent cause of pulmonary rales, particularly in its advanced stages. When the heart fails to pump blood efficiently, blood can back up into the veins leading to the lungs, causing fluid to leak into the alveolar spaces. This condition, known as pulmonary congestion, results in bilateral (both sides) or basal (lower lung fields) rales. Patients with heart failure often experience additional symptoms such as fatigue, swelling in the legs, and difficulty breathing, especially when lying down. The rales in heart failure are often described as fine or coarse crackles, depending on the extent of fluid accumulation.
Pulmonary edema, a condition characterized by the accumulation of fluid in the lungs, is a direct cause of rales and is often a complication of heart failure or other cardiac conditions. However, pulmonary edema can also result from non-cardiac causes, such as acute respiratory distress syndrome (ARDS), high altitude exposure, or drug toxicity. In pulmonary edema, the fluid overwhelms the alveoli, leading to widespread crackling sounds that are often described as "wet" or "bubbly." This condition is a medical emergency, as it severely impairs oxygen exchange and can rapidly progress to respiratory failure if not treated promptly.
In addition to these conditions, acute bronchitis and chronic obstructive pulmonary disease (COPD) can also cause rales, though they are less commonly associated with this finding. Acute bronchitis, often viral in origin, can lead to mucus buildup in the airways, sometimes producing fine crackles. In COPD, particularly during exacerbations, increased mucus production and airway inflammation may result in scattered rales, though wheezing is more typical. Understanding the underlying cause of rales is crucial for appropriate management, as treatments vary significantly depending on whether the condition is infectious, cardiac, or related to fluid overload.
Lastly, interstitial lung diseases (ILDs), such as idiopathic pulmonary fibrosis, can cause rales due to scarring and stiffening of the lung tissue. In these conditions, the crackles are often fine and persistent, reflecting the chronic nature of the disease. ILDs are progressive and require specialized treatment, including medications to slow disease progression and supportive care to manage symptoms. Recognizing the specific characteristics of rales—their location, timing (during inhalation or exhalation), and quality—can help clinicians narrow down the differential diagnosis and initiate targeted therapy.
Understanding the Unique Vocalizations: How Does a Goat Sound?
You may want to see also
![]()
Timing of Rales: Assessing inspiratory vs. expiratory rales and their clinical implications
Pulmonary rales, often described as crackles, are abnormal lung sounds that can provide crucial insights into underlying respiratory conditions. The timing of these sounds—whether they occur during inspiration or expiration—is a key factor in their clinical interpretation. Inspiratory rales are heard as the patient inhales and are typically associated with conditions that cause fluid or debris to accumulate in the alveoli or small airways. These sounds are often described as brief, discontinuous, and high-pitched, resembling the rustling of leaves or Velcro being pulled apart. Inspiratory rales are commonly observed in conditions such as pneumonia, pulmonary edema, or interstitial lung disease, where the airways are filled with fluid or inflammatory exudate during the inspiratory phase.
In contrast, expiratory rales are heard during exhalation and are less common than inspiratory rales. They are often associated with conditions that cause airway obstruction or inflammation, such as chronic obstructive pulmonary disease (COPD), asthma, or bronchiectasis. Expiratory rales may sound similar to inspiratory rales but are distinguished by their timing. The presence of expiratory rales suggests that the airways are narrowed or filled with mucus or debris during the expiratory phase, leading to turbulent airflow and the characteristic crackling sounds.
Assessing the timing of rales is critical for differential diagnosis. Inspiratory rales often indicate alveolar or interstitial involvement, pointing to conditions like acute respiratory distress syndrome (ARDS) or congestive heart failure, where fluid accumulates in the lungs. On the other hand, expiratory rales are more suggestive of obstructive airway diseases, such as COPD or cystic fibrosis, where mucus plugging or bronchial inflammation plays a central role. Clinicians must also consider the distribution and intensity of rales, as these factors further refine the diagnostic possibilities.
The clinical implications of inspiratory versus expiratory rales extend to treatment strategies. For example, inspiratory rales in a patient with pulmonary edema may prompt the use of diuretics to reduce fluid overload, while expiratory rales in a patient with asthma may indicate the need for bronchodilators or inhaled corticosteroids to alleviate airway obstruction. Additionally, the timing of rales can help monitor disease progression or response to therapy, as changes in the pattern or intensity of sounds may reflect improvements or worsening of the underlying condition.
In practice, auscultation should be performed carefully, with attention to the patient’s breathing cycle, to accurately identify whether rales are inspiratory or expiratory. Using a stethoscope, the clinician should listen for the onset and duration of the sounds relative to the respiratory phase. This distinction, combined with other clinical findings such as patient history, physical examination, and imaging studies, enables a more precise diagnosis and tailored management approach. Understanding the timing of rales is thus an essential skill for healthcare providers in evaluating and treating respiratory disorders effectively.
Sound Localization: A Vital Survival Skill in Nature's Complex World
You may want to see also
Frequently asked questions
Pulmonary rales sound like crackling, bubbling, or rattling noises in the lungs, often described as similar to the sound of opening a Velcro strap or walking on fresh snow.
Pulmonary rales are typically heard in the lower lung fields, especially during inspiration, but can also be present in other areas depending on the underlying condition.
Pulmonary rales are caused by fluid, mucus, or air in the alveoli or small airways, which creates turbulence as air moves through the lungs during breathing.
Pulmonary rales are crackling or bubbling sounds, while wheezing is a high-pitched whistling sound caused by narrowed airways, often associated with conditions like asthma.