Taking an ultrasound of the breast, also known as a breast ultrasound, is a non-invasive imaging technique used to examine breast tissue for abnormalities, such as lumps, cysts, or tumors. During the procedure, a trained technician or radiologist applies a water-based gel to the breast and uses a small handheld device called a transducer to emit high-frequency sound waves. These sound waves penetrate the breast tissue, creating real-time images on a monitor, allowing the healthcare provider to assess the size, shape, and characteristics of any detected masses. Breast ultrasounds are often used as a complementary tool to mammography, particularly for women with dense breast tissue or to further evaluate findings from a physical exam or mammogram. The procedure is painless, typically takes 15-30 minutes, and does not involve radiation exposure, making it a safe and effective diagnostic option.
| Characteristics | Values |
|---|---|
| Purpose | To visualize breast tissue, detect abnormalities, and guide biopsies. |
| Equipment | High-frequency linear transducer (7-14 MHz), ultrasound machine. |
| Patient Position | Supine (lying flat on back) or seated, with arm raised above the head. |
| Gel Application | Ultrasound gel applied to the breast to ensure proper contact. |
| Scanning Technique | Transverse and sagittal planes to assess all breast quadrants. |
| Imaging Focus | Evaluate masses, cysts, lymph nodes, and vascularity. |
| Compression | Gentle compression applied to displace tissue and improve visualization. |
| Contrast Enhancement | Optional use of contrast agents for advanced imaging (e.g., CEUS). |
| Duration | Typically 15-30 minutes per breast. |
| Indications | Palpable lumps, pain, screening in dense breasts, follow-up of abnormalities. |
| Limitations | Operator-dependent, may not detect microcalcifications (X-ray is better). |
| Safety | Non-invasive, no radiation exposure. |
| Post-Procedure | No downtime; patient can resume normal activities immediately. |
| Reporting | Radiologist interprets images and provides a detailed report. |
| Follow-Up | Further tests (e.g., biopsy) may be recommended based on findings. |
Explore related products






What You'll Learn
- Preparation: Patient positioning, exposed chest, warm gel application, and transducer selection for optimal imaging
- Transducer Technique: Gentle pressure, sweeping motions, and angle adjustments to capture all breast tissue
- Imaging Planes: Sagittal, transverse, and axial views to assess lesions and structures comprehensively
- Lesion Evaluation: Size, shape, margins, echogenicity, and vascularity analysis using Doppler techniques
- Documentation: Clear labeling, measurements, and annotations for accurate reporting and follow-up comparisons
![]()
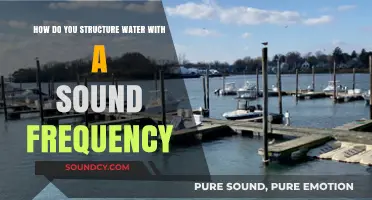
Preparation: Patient positioning, exposed chest, warm gel application, and transducer selection for optimal imaging
Proper patient positioning is the cornerstone of a successful breast ultrasound. The patient should lie in a supine position, with the arm on the side of the breast being examined raised above the head. This position helps to flatten the breast tissue, allowing for better visualization and reducing the risk of missing any abnormalities. For obese patients or those with large breasts, placing a rolled towel under the shoulder can further enhance tissue flattening and improve image quality. Ensuring the patient is comfortable is equally important, as tension can cause muscle contractions that obscure the view.
Exposing the chest adequately is a critical yet often overlooked step. The entire breast, including the axillary tail and the axilla, should be accessible. Remove any clothing or jewelry that might interfere with the scan. For modesty, a drape can be used to cover areas not being imaged. It’s essential to explain the process to the patient beforehand to alleviate anxiety and ensure cooperation. Clear communication can also help the patient understand why full exposure is necessary for a comprehensive evaluation.
The application of warm gel is more than just a procedural step—it’s a key to optimal imaging. Cold gel can cause discomfort and make the patient tense, degrading image quality. Warming the gel to body temperature (around 37°C) ensures patient comfort and improves acoustic coupling. Apply a generous amount of gel to the transducer and the breast surface, avoiding air pockets that can distort the image. For patients with sensitive skin, hypoallergenic gel should be used to prevent irritation.
Transducer selection is the final piece of the preparation puzzle. A high-frequency linear array transducer (7–14 MHz) is typically used for breast imaging, as it provides high-resolution images of superficial structures. For deeper tissue penetration in larger breasts, a lower frequency (5–10 MHz) curved array transducer may be more appropriate. The choice depends on the patient’s anatomy and the clinical question. Proper handling of the transducer, including maintaining light, even pressure, ensures consistent imaging without causing discomfort.
In summary, meticulous preparation—from patient positioning to transducer selection—lays the foundation for an accurate and efficient breast ultrasound. Each step, though seemingly minor, plays a significant role in optimizing image quality and patient experience. Attention to these details not only enhances diagnostic accuracy but also fosters trust and cooperation between the sonographer and the patient.
Mastering Your Guitar Tone: Essential Tips to Adjust Sound Perfectly
You may want to see also
Explore related products






![]()
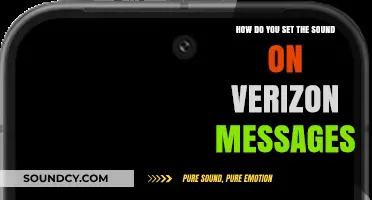
Transducer Technique: Gentle pressure, sweeping motions, and angle adjustments to capture all breast tissue
Breast ultrasound imaging relies heavily on the sonographer’s transducer technique to ensure comprehensive tissue visualization. Gentle, consistent pressure is paramount to eliminate air gaps between the transducer and the skin, which can distort images or create artifacts. Apply enough force to maintain contact but avoid excessive pressure that might compress tissue and obscure abnormalities. This balance is particularly critical when examining denser breast tissue or areas near the chest wall, where subtle lesions can easily be missed.
Sweeping motions are the next critical component, enabling the sonographer to cover the entire breast systematically. Begin at the nipple and move outward in a radial pattern, overlapping each pass slightly to avoid gaps. For larger breasts, divide the area into quadrants (upper outer, upper inner, lower outer, lower inner) and scan each section methodically. Incorporate lateral and medial sweeps to capture axillary tail tissue, a common site for metastatic lymph nodes. Speed matters: move the transducer slowly enough to allow real-time image interpretation but efficiently to minimize patient discomfort.
Angle adjustments are equally vital for assessing tissue depth and characterizing lesions. Tilt the transducer slightly to visualize structures at different planes, particularly when evaluating masses or assessing posterior acoustic enhancement. For example, a 45-degree angle can help differentiate a cyst’s smooth walls from a solid tumor’s irregular margins. In obese patients or those with dense tissue, steep angles may be necessary to penetrate deeper layers without losing resolution. Practice adjusting angles in real-time to correlate findings with physical exam landmarks.
Mastering these techniques requires deliberate practice and anatomical familiarity. Use anatomical markers (e.g., ribs, clavicle) to orient scans and ensure consistency. For patients with prior surgeries or implants, modify pressure and angles to accommodate scar tissue or altered anatomy. Always document technical challenges (e.g., "limited views due to patient discomfort") to justify image limitations. With experience, sonographers develop a rhythm that balances speed, pressure, and angulation to maximize diagnostic yield while maintaining patient comfort.
Can Sound Travel Through a Vacuum? Unraveling the Science Behind Silence
You may want to see also
Explore related products




![]()
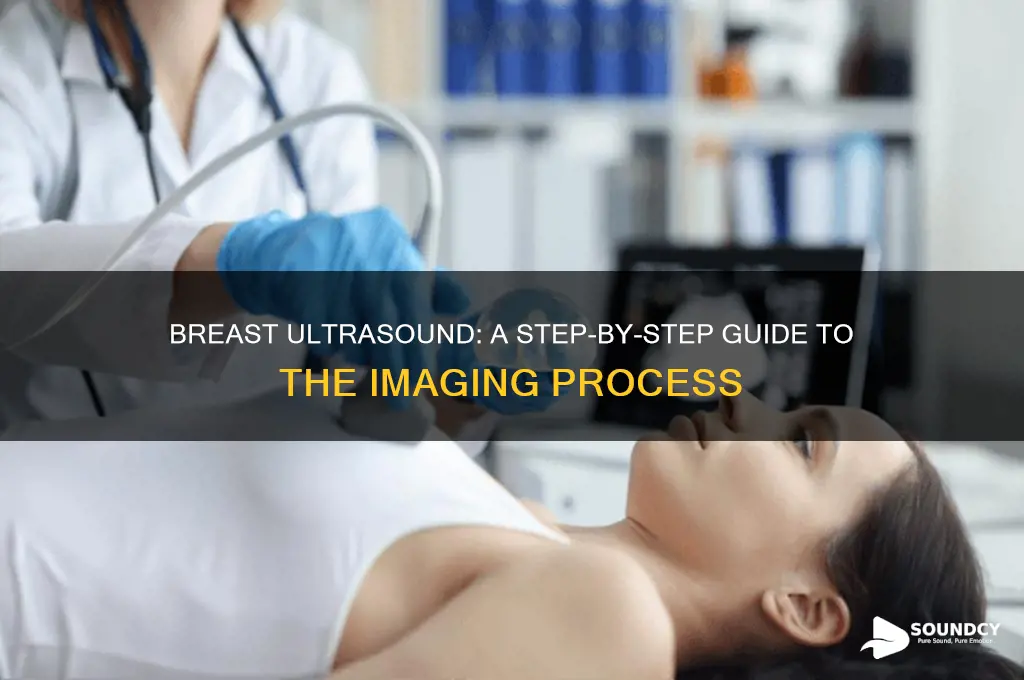
Imaging Planes: Sagittal, transverse, and axial views to assess lesions and structures comprehensively
Breast ultrasound imaging relies heavily on the strategic use of sagittal, transverse, and axial planes to evaluate lesions and anatomical structures thoroughly. Each plane offers a unique perspective, contributing to a comprehensive assessment. The sagittal plane, for instance, divides the breast into left and right sections, providing a detailed view of the cooperative relationship between the lesion and the nipple-areolar complex. This orientation is particularly useful for assessing the depth and extension of abnormalities in relation to the chest wall.
In contrast, the transverse plane offers a cross-sectional view, slicing the breast horizontally. This perspective is invaluable for evaluating the size, shape, and margins of lesions, as well as their relationship to surrounding tissues, such as the pectoralis muscle or skin. Radiologists often use this plane to measure lesion dimensions accurately, with a typical transducer frequency of 7-14 MHz for optimal resolution. For patients over 40, this plane can be crucial in distinguishing between benign and malignant masses, especially when combined with color Doppler to assess vascularity.
The axial plane, though less commonly used in breast ultrasound, provides a top-down view, parallel to the chest wall. This orientation is beneficial for assessing the overall architecture of the breast, including ductal distribution and the presence of diffuse abnormalities. While not a primary diagnostic plane, it can offer supplementary information, particularly in cases of extensive disease or when evaluating implant integrity in augmented breasts.
To maximize diagnostic accuracy, sonographers should systematically scan all three planes. Begin with the sagittal plane to localize the lesion relative to landmarks, followed by the transverse plane for detailed characterization. Incorporate the axial plane as needed for broader context. Practical tips include using a generous amount of gel to minimize artifact, adjusting the transducer angle to optimize visualization, and ensuring patient comfort to facilitate thorough examination. This multi-planar approach ensures no critical detail is overlooked, enhancing both diagnostic confidence and patient outcomes.
Why 'Apt' Sounds Familiar: Unraveling the Word's Ubiquity and Appeal
You may want to see also
Explore related products





![]()
Lesion Evaluation: Size, shape, margins, echogenicity, and vascularity analysis using Doppler techniques
Breast ultrasound is a critical tool for evaluating lesions, offering detailed insights into their characteristics without exposing patients to ionizing radiation. When assessing a lesion, the radiologist focuses on five key features: size, shape, margins, echogenicity, and vascularity. Each of these elements provides unique information that helps differentiate between benign and malignant findings. For instance, a well-defined, oval lesion with smooth margins and uniform echogenicity is more likely benign, while an irregular, hypoechoic mass with angular margins and increased vascularity raises suspicion for malignancy.
Size and Shape Analysis: Begin by measuring the lesion’s longest diameter, width, and depth using calipers. Document the size in millimeters, as lesions larger than 10 mm often warrant further investigation. Shape is equally important—benign lesions tend to be oval or round, while malignant ones may appear irregular or taller than wide (a sign known as the "orientation ratio"). Use the "ABCDE" rule adapted for ultrasound: asymmetry, border irregularity, circularity (lack thereof), diameter (>1 cm), and extension into surrounding tissue. For example, a 15 mm irregular mass with an orientation ratio greater than 1:1 should prompt biopsy consideration.
Margins and Echogenicity Evaluation: Margins describe the lesion’s boundary with surrounding tissue. Well-defined, smooth margins suggest benignity, whereas microlobulated, indistinct, or spiculated margins are concerning. Echogenicity refers to the lesion’s brightness relative to adjacent tissue. Hypoechoic lesions (darker than surrounding tissue) are more commonly malignant, while hyperechoic or isoechoic lesions are typically benign. However, exceptions exist—some benign fibroadenomas can be hypoechoic, so correlation with other features is essential.
Vascularity Analysis Using Doppler Techniques: Doppler ultrasound assesses blood flow within the lesion, a critical indicator of malignancy. Use color Doppler to identify vascular patterns, followed by spectral Doppler for detailed analysis. Malignant lesions often exhibit peripheral, chaotic, or penetrating vessels, while benign lesions show central, linear, or absent vascularity. For instance, a hypoechoic mass with peripheral vascularity on color Doppler and low-resistance arterial flow on spectral Doppler strongly suggests malignancy. Practical tip: Adjust the Doppler scale to 50–100 cm/s for optimal sensitivity without oversaturating the image.
Integrating Findings for Accurate Diagnosis: Combining size, shape, margins, echogenicity, and vascularity creates a comprehensive profile of the lesion. For example, a 12 mm irregular, hypoechoic mass with microlobulated margins and peripheral vascularity would score high on the Breast Imaging Reporting and Data System (BI-RADS) scale, indicating a high probability of malignancy. Conversely, a 7 mm round, isoechoic lesion with smooth margins and no vascularity would likely be categorized as benign. Always correlate ultrasound findings with clinical history, mammography, and MRI when available for a definitive diagnosis.
Master Keyboard Sound Effects: Creative Techniques for Typing Noises
You may want to see also
Explore related products






![]()
Documentation: Clear labeling, measurements, and annotations for accurate reporting and follow-up comparisons
Accurate documentation is the backbone of effective breast ultrasound, transforming images into actionable insights. Clear labeling, precise measurements, and detailed annotations ensure consistency in reporting, enabling radiologists to track changes over time and make informed decisions. Without this structured approach, critical details can be overlooked, leading to misinterpretation or delayed diagnoses. For instance, labeling the quadrant or clock position of a lesion (e.g., "10 o’clock, upper outer quadrant") provides spatial context, while noting the size (e.g., "1.2 cm x 0.8 cm") establishes a baseline for future comparisons. This level of specificity is non-negotiable in a field where millimeters matter.
Consider the process as a three-step protocol: first, label each image with patient identifiers, study date, and probe orientation (e.g., "transverse view, left breast"). Second, measure key parameters—lesion size, margins, and vascularity—using calipers or software tools, ensuring consistency in technique (e.g., measuring the longest axis first). Third, annotate findings with descriptors like "well-circumscribed hypoechoic mass" or "posterior acoustic enhancement," adhering to standardized terminology (e.g., BI-RADS lexicon). These steps eliminate ambiguity, allowing follow-up studies to align precisely with prior data. For example, a 2021 study in *Ultrasound in Medicine & Biology* found that standardized annotations reduced diagnostic discrepancies by 30% in multi-reader assessments.
The persuasive argument for meticulous documentation lies in its impact on patient outcomes. In breast cancer screening, a misdocumented lesion size or location can lead to incorrect staging or treatment planning. For instance, a 5 mm discrepancy in measurement might classify a lesion as benign (BI-RADS 2) instead of requiring biopsy (BI-RADS 4a). Similarly, omitting annotations about vascularity or architectural distortion could delay the detection of angiogenesis, a hallmark of malignancy. By prioritizing clarity and precision, sonographers act as stewards of patient safety, ensuring that every scan contributes meaningfully to the diagnostic journey.
Comparatively, breast ultrasound documentation differs from other imaging modalities in its reliance on real-time interpretation and operator skill. Unlike mammography, where positioning is standardized, ultrasound requires dynamic adjustments, making annotations even more critical. For example, noting the depth of a lesion (e.g., "2.5 cm from skin surface") aids in correlating findings with physical exams or biopsies. This level of detail is particularly valuable in dense breasts, where ultrasound serves as a complementary tool to mammography. By embracing a structured documentation framework, practitioners bridge the gap between technical proficiency and clinical utility.
Practically, integrating these principles into daily practice requires training and tools. Software with built-in measurement templates and annotation libraries streamlines the process, reducing the risk of human error. For instance, using color-coded labels for different findings (e.g., green for cysts, red for solid masses) enhances visual clarity. Additionally, adopting a checklist approach—verifying labels, measurements, and annotations before finalizing the report—ensures nothing is overlooked. For trainees, peer review sessions focused on documentation quality can reinforce best practices. Ultimately, the goal is to create a record that stands the test of time, enabling seamless follow-up and confident decision-making.
Exploring the Unique Sounds and Rhythms of Kyrgyz Language
You may want to see also
Frequently asked questions
A breast ultrasound is a non-invasive imaging test that uses sound waves to create images of the breast tissue. It is performed to evaluate lumps, pain, or abnormalities detected during a physical exam or mammogram, and to differentiate between fluid-filled cysts and solid masses.
There is minimal preparation required for a breast ultrasound. Wear comfortable clothing, and avoid applying lotions, powders, or deodorants on the chest area, as these can interfere with the imaging process.
During the procedure, you will lie on your back or side, and a technician will apply a gel to your breast. A small handheld device called a transducer is then moved over the area, emitting sound waves to create real-time images on a monitor. The process is painless and typically takes 15–30 minutes.
Breast ultrasound is safe and does not involve radiation or injections. There are no known risks or side effects, making it a preferred imaging method for pregnant women and individuals who cannot undergo mammograms.