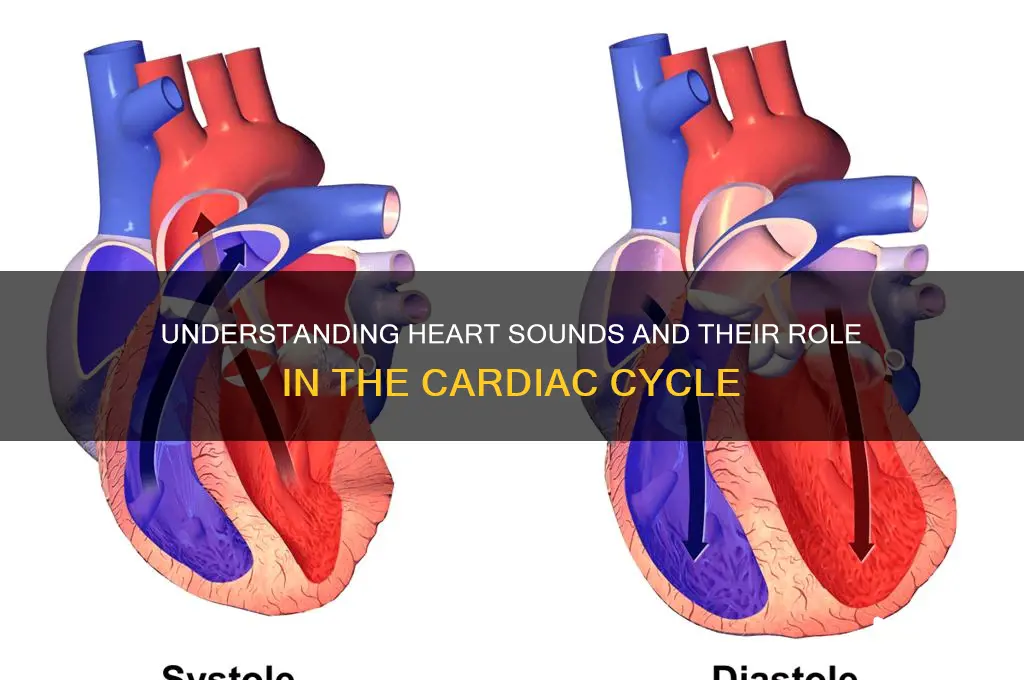
Heart sounds are directly related to the cardiac cycle, which consists of the sequential phases of the heart’s pumping action: systole (contraction) and diastole (relaxation). The first heart sound (S1), often described as lub, occurs at the beginning of systole, coinciding with the closure of the mitral and tricuspid valves as the ventricles contract to eject blood. The second heart sound (S2), or dub, marks the start of diastole, corresponding to the closure of the aortic and pulmonary valves as the ventricles finish ejecting blood and begin to relax. These sounds are produced by the turbulent blood flow and valve movements during the cardiac cycle, providing clinicians with valuable insights into the heart’s function and timing of its phases. Additional heart sounds, such as S3 and S4, may indicate pathologies or changes in ventricular filling dynamics, further highlighting the intimate connection between heart sounds and the cardiac cycle.
| Characteristics | Values |
|---|---|
| Heart Sound S1 | Marks the beginning of systole; caused by closure of the mitral and tricuspid valves (AV valves); associated with the onset of ventricular contraction and isometric contraction phase. |
| Heart Sound S2 | Marks the beginning of diastole; caused by closure of the aortic and pulmonary valves (semilunar valves); associated with the end of ventricular ejection and the start of ventricular relaxation. |
| Timing of S1 | Occurs at the end of the QRS complex on the ECG, coinciding with the start of ventricular contraction. |
| Timing of S2 | Occurs slightly after the T wave on the ECG, coinciding with the end of ventricular ejection. |
| Duration of S1 | Typically shorter than S2, lasting about 0.1-0.12 seconds. |
| Duration of S2 | Slightly longer than S1, lasting about 0.12-0.16 seconds; may split into two components (A2 and P2) due to differences in closure times of the aortic and pulmonary valves. |
| Intensity of S1 | Generally louder than S2, especially in children and young adults. |
| Intensity of S2 | May vary; often softer than S1 but can be accentuated in certain conditions (e.g., pulmonary hypertension). |
| Physiological Splitting | Normal splitting of S2 occurs during inspiration due to lower intrathoracic pressure, delaying pulmonary valve closure relative to the aortic valve. |
| Pathological Splitting | Abnormal splitting of S2 can indicate conditions like left bundle branch block or atrial septal defect. |
| Third Heart Sound (S3) | Occurs in early diastole; associated with rapid ventricular filling; may be normal in children and athletes but pathological in adults (e.g., heart failure). |
| Fourth Heart Sound (S4) | Occurs in late diastole; associated with atrial contraction and increased ventricular stiffness; often pathological (e.g., hypertension, aortic stenosis). |
| Relationship to ECG | S1 aligns with the onset of the QRS complex, while S2 occurs after the T wave; S3 and S4, if present, occur before the next P wave. |
| Clinical Significance | Abnormalities in heart sounds (e.g., murmurs, extra sounds) can indicate valvular disease, myocardial dysfunction, or other cardiac conditions. |
Explore related products






What You'll Learn
- First Heart Sound (S1): Marks mitral/tricuspid valve closure, beginning systole, lub sound
- Second Heart Sound (S2): Indicates aortic/pulmonic valve closure, end systole, dub sound
- Heart Murmur Timing: Abnormal sounds during systole/diastole, linked to valve issues
- Third Heart Sound (S3): Rare, early diastolic sound, suggests heart failure
- Fourth Heart Sound (S4): Rare, late diastolic sound, linked to stiff ventricles
![]()
First Heart Sound (S1): Marks mitral/tricuspid valve closure, beginning systole, lub sound
The first heart sound, often described as the "lub" in the familiar "lub-dub" rhythm, is a critical marker in the cardiac cycle. It signifies the closure of the mitral and tricuspid valves, which occurs at the onset of systole. This sound is produced when the atrioventricular (AV) valves snap shut, preventing blood from flowing back into the atria as the ventricles begin to contract. Clinicians rely on this sound to assess the timing and efficiency of ventricular contraction, making it a cornerstone of cardiac auscultation.
Analyzing the first heart sound (S1) reveals its dual significance: it not only marks the transition from diastole to systole but also provides insights into valve function. The intensity and quality of S1 can indicate whether the mitral and tricuspid valves are closing properly. For instance, a soft or muffled S1 may suggest valve dysfunction or stenosis, while a split sound could indicate delayed closure of one valve relative to the other. Understanding these nuances is essential for diagnosing conditions like mitral valve prolapse or tricuspid regurgitation.
To effectively identify S1, healthcare providers use a stethoscope placed over the mitral and tricuspid valve areas. The sound is best heard at the apex of the heart (mitral area) and the left lower sternal border (tricuspid area). Patients should be in a relaxed position, ideally lying on their left side, to optimize sound detection. For medical students or practitioners, practicing auscultation on diverse patient populations—ranging from children (where S1 is often louder due to thinner chest walls) to the elderly (where sounds may be softer due to calcification)—can enhance diagnostic accuracy.
A practical tip for distinguishing S1 from other sounds is to correlate it with the carotid pulse. S1 coincides with the palpable peak of the pulse, reinforcing its role as the beginning of systole. This synchronization is particularly useful in teaching settings or when training new clinicians. Additionally, using visual aids like phonocardiograms can help learners visualize the relationship between S1 and the cardiac cycle, bridging the gap between theory and practice.
In conclusion, the first heart sound is more than just a "lub"—it’s a vital indicator of cardiac health and function. By understanding its timing, characteristics, and clinical implications, healthcare professionals can better diagnose and manage cardiovascular conditions. Whether in a bustling emergency department or a quiet clinic, mastering the nuances of S1 is an indispensable skill for anyone involved in cardiac care.
Does Fitbit Blaze Make Sound? Exploring Its Audio Features and Alerts
You may want to see also
Explore related products






![]()
Second Heart Sound (S2): Indicates aortic/pulmonic valve closure, end systole, dub sound
The second heart sound (S2) is a critical marker in the cardiac cycle, signaling the end of systole and the closure of the aortic and pulmonic valves. This distinct "dub" sound is produced as blood flow from the ventricles to the aorta and pulmonary artery abruptly stops, causing these valves to snap shut. Clinicians rely on S2 to assess the timing and efficiency of ventricular ejection, making it a vital component of auscultation. For instance, a widened splitting of S2 can indicate delayed closure of the pulmonic valve, often seen in conditions like atrial septal defect or right bundle branch block.
Analyzing S2 requires attention to its intensity, quality, and timing. Normally, S2 is softer than the first heart sound (S1) but should be clearly audible. A loud or "snapping" S2 may suggest pulmonary hypertension, while a muffled sound could indicate valve dysfunction. The split nature of S2—with the aortic component closing slightly before the pulmonic—is physiologic in inspiration and disappears in expiration. However, a persistent split S2 warrants investigation, as it may reflect underlying cardiac abnormalities.
To effectively evaluate S2, use a diaphragm stethoscope placed over the pulmonic area (second left intercostal space) and the aortic area (third right intercostal space). Listen during both inspiration and expiration to assess splitting. For pediatric patients, ensure the stethoscope bell is used for lower-pitched sounds, while adults typically require the diaphragm. Document the characteristics of S2 alongside other heart sounds to provide a comprehensive cardiac assessment.
In practical terms, understanding S2 is essential for differentiating benign variations from pathological conditions. For example, a wide and fixed split S2 in a young adult might prompt further imaging, such as an echocardiogram, to rule out congenital heart defects. Conversely, recognizing a normal split S2 in a healthy individual prevents unnecessary diagnostic procedures. By mastering the nuances of S2, healthcare providers can enhance their diagnostic accuracy and patient care.
Do Roof Rats Make Sounds? Understanding Their Noises and Behavior
You may want to see also
Explore related products






![]()
Heart Murmur Timing: Abnormal sounds during systole/diastole, linked to valve issues
Heart murmurs are abnormal sounds that occur during the cardiac cycle, often signaling underlying valve issues. These sounds are typically heard during systole (when the heart contracts) or diastole (when the heart relaxes), and their timing is crucial for diagnosis. For instance, a systolic murmur may indicate problems like aortic stenosis or mitral regurgitation, while a diastolic murmur could point to conditions such as aortic regurgitation or mitral stenosis. Understanding the timing of these murmurs helps healthcare providers pinpoint the affected valve and the nature of the dysfunction.
To identify a heart murmur, clinicians use a stethoscope to listen for sounds that differ from the normal "lub-dub" of the cardiac cycle. Systolic murmurs occur between S1 (the first heart sound) and S2 (the second heart sound), while diastolic murmurs are heard between S2 and the next S1. For example, a mid-systolic murmur is often associated with mitral valve prolapse, whereas a late-peaking systolic murmur may suggest hypertrophic cardiomyopathy. Recognizing these patterns requires practice and a systematic approach to auscultation, starting at the mitral area and moving to the aortic, pulmonic, and tricuspid areas.
The duration and intensity of a murmur also provide valuable clues. A systolic murmur that increases in intensity (crescendo) and then decreases (decrescendo) is characteristic of aortic stenosis. Conversely, a diastolic murmur that is high-pitched and short may indicate aortic regurgitation. Clinicians grade murmurs on a scale of 1 to 6, with grade 1 being barely audible and grade 6 being heard with the stethoscope slightly off the chest. This grading system, combined with timing, helps differentiate benign murmurs (innocent murmurs) from pathological ones requiring further investigation.
Practical tips for detecting heart murmurs include ensuring the patient is in a quiet environment and using proper stethoscope technique. For children or anxious patients, having them sit upright or lean forward can improve sound clarity. If a murmur is suspected, additional tests like echocardiography or Doppler studies may be necessary to confirm the diagnosis. Early detection and accurate timing of murmurs can lead to timely interventions, such as valve repair or medication management, preventing complications like heart failure or arrhythmias.
In summary, the timing of heart murmurs during systole or diastole is a critical diagnostic tool for identifying valve abnormalities. By correlating murmur characteristics with the cardiac cycle, healthcare providers can localize the issue and guide appropriate treatment. Whether in a clinical or educational setting, mastering the art of auscultation and understanding murmur timing is essential for effective cardiovascular care.
Crafting Rocket Sounds: A Step-by-Step Guide to Authentic Effects
You may want to see also
Explore related products






![]()
Third Heart Sound (S3): Rare, early diastolic sound, suggests heart failure
The third heart sound, or S3, is a subtle yet significant marker in the cardiac cycle, often described as a low-pitched, brief sound occurring in early diastole. Unlike the ubiquitous S1 and S2, which correspond to mitral and tricuspid valve closure and aortic and pulmonary valve closure, respectively, S3 is rare and typically absent in healthy adults. Its presence, however, can signal underlying cardiac dysfunction, particularly in the context of heart failure. This sound arises from rapid ventricular filling during early diastole, when increased blood volume or decreased compliance causes the ventricle to expand abruptly, vibrating the ventricular walls. Clinicians must recognize S3 as a red flag, prompting further investigation into the patient’s cardiac health.
To identify S3, auscultation should be performed with the patient in the left lateral decubitus position, using the bell of the stethoscope over the cardiac apex. The sound is best heard during expiration, as this phase of respiration enhances early diastolic filling. S3 is often described as a "ventricular gallop" when paired with S4, creating a rhythm akin to the phrase "Kentucky" (S1-S2 as "Ken" and S3-S4 as "tuck-y"). However, in isolation, S3 is a solitary, soft sound that requires a trained ear to detect. Its timing is crucial: occurring 0.12 to 0.18 seconds after S2, it distinguishes itself from other diastolic sounds like mitral regurgitation or opening snap.
The clinical implications of S3 are profound, particularly in patients over 40 years old or those with risk factors for heart failure. In younger individuals, S3 may be physiological, especially in athletes or pregnant women, where increased blood volume and cardiac output are normal. However, in older adults or those with hypertension, diabetes, or coronary artery disease, S3 is pathological, often indicating reduced ventricular compliance or elevated filling pressures. Studies show that S3 is present in approximately 50% of patients with symptomatic heart failure, making it a valuable diagnostic tool when combined with other findings like elevated BNP levels or echocardiographic evidence of reduced ejection fraction.
Managing patients with S3 requires a systematic approach. Initial steps include optimizing heart failure therapies, such as diuretics to reduce volume overload or ACE inhibitors to improve ventricular compliance. Lifestyle modifications, including sodium restriction and fluid management, are essential. For example, patients with New York Heart Association (NYHA) Class II or III symptoms may benefit from a daily sodium intake of 2,000 mg or less. Regular monitoring of weight, blood pressure, and symptoms is critical to assess treatment efficacy. If S3 persists despite therapy, advanced interventions like implantable cardioverter-defibrillators (ICDs) or cardiac resynchronization therapy (CRT) may be considered, particularly in patients with reduced ejection fraction and prolonged QRS duration.
In conclusion, while S3 is a rare finding, its detection demands attention and action. It serves as an early warning sign of ventricular dysfunction, often preceding overt symptoms of heart failure. By understanding its pathophysiology, mastering auscultation techniques, and implementing targeted interventions, clinicians can improve patient outcomes and potentially halt disease progression. S3 is not merely a sound but a call to action, urging a comprehensive approach to cardiac care.
Peeing After Sounding: Essential Aftercare Tips for Safe Urethral Play
You may want to see also
Explore related products






![]()
Fourth Heart Sound (S4): Rare, late diastolic sound, linked to stiff ventricles
The fourth heart sound, or S4, is a subtle yet significant marker of cardiac function, often overlooked due to its rarity and low amplitude. It occurs during late diastole, just before the first heart sound (S1), and is best heard at the cardiac apex with the patient in the left lateral decubitus position. Unlike the more common S1 and S2, which are associated with valve closure, S4 is linked to the mechanical properties of the ventricles themselves. Its presence is a red flag, signaling increased ventricular stiffness, a condition that impairs the heart’s ability to fill properly during diastole.
To understand S4, consider the cardiac cycle’s diastolic phase. Normally, blood flows passively from the atria into the ventricles as they relax. However, in a stiff ventricle, this process is compromised. The myocardium loses its compliance, requiring higher atrial pressures to push blood into the ventricle. This mechanical strain generates the low-frequency vibration we hear as S4. Clinically, it is often described as a soft, rumbling sound, distinct from the sharper tones of S1 and S2. Patients with S4 may be asymptomatic, but its detection warrants further investigation, as it is frequently associated with conditions like hypertension, left ventricular hypertrophy, or ischemic heart disease.
Diagnosing S4 requires precision. A standard stethoscope may not suffice; using a diaphragm placed firmly on the chest wall, with the patient in a position that maximizes sound transmission, is critical. The sound is more audible during expiration and in the absence of background noise. For healthcare providers, recognizing S4 is a skill honed through practice and familiarity with its unique characteristics. It is not a benign finding—its presence often correlates with elevated left ventricular end-diastolic pressure, a predictor of heart failure.
From a treatment perspective, addressing S4 involves managing the underlying cause of ventricular stiffness. For hypertensive patients, antihypertensive medications like ACE inhibitors or beta-blockers can reduce afterload and improve ventricular compliance. In cases of ischemia, revascularization strategies such as PCI or CABG may be necessary. Lifestyle modifications, including weight management, sodium restriction, and regular exercise, play a pivotal role in mitigating the progression of ventricular stiffness. Early intervention is key, as untreated stiffness can lead to diastolic dysfunction and, ultimately, heart failure.
In summary, the fourth heart sound is a rare but critical indicator of ventricular health. Its detection demands clinical acumen and a systematic approach to auscultation. By understanding its pathophysiology and associated conditions, healthcare providers can initiate timely interventions to prevent long-term cardiac complications. S4 serves as a reminder that even the subtlest sounds can reveal profound insights into the heart’s function.
Are All Valid Arguments Sound? Exploring Logic and Truth
You may want to see also
Frequently asked questions
Heart sounds are the noises produced by the closing of heart valves and the contraction of cardiac muscles. The two primary heart sounds, S1 and S2, are directly related to the cardiac cycle. S1 (lub) occurs at the beginning of systole when the mitral and tricuspid valves close, while S2 (dub) occurs at the start of diastole when the aortic and pulmonary valves close.
S1 corresponds to the closure of the mitral and tricuspid valves at the beginning of ventricular contraction (systole). This marks the transition from diastole to systole, as blood is prevented from flowing back into the atria, and the ventricles begin to eject blood into the aorta and pulmonary artery.
S2 is caused by the closure of the aortic and pulmonary valves at the end of ventricular systole, marking the beginning of diastole. This occurs when ventricular pressure falls below the pressure in the aorta and pulmonary artery, preventing backflow and allowing the ventricles to relax and fill with blood.
Yes, additional sounds like S3 and S4 can occur in certain conditions. S3 is a low-pitched sound heard in early diastole, often associated with increased blood volume or decreased compliance of the ventricles. S4 is a presystolic sound caused by atrial contraction against stiff ventricles, often seen in hypertensive heart disease. These sounds are not part of the normal cardiac cycle but indicate underlying cardiac issues.