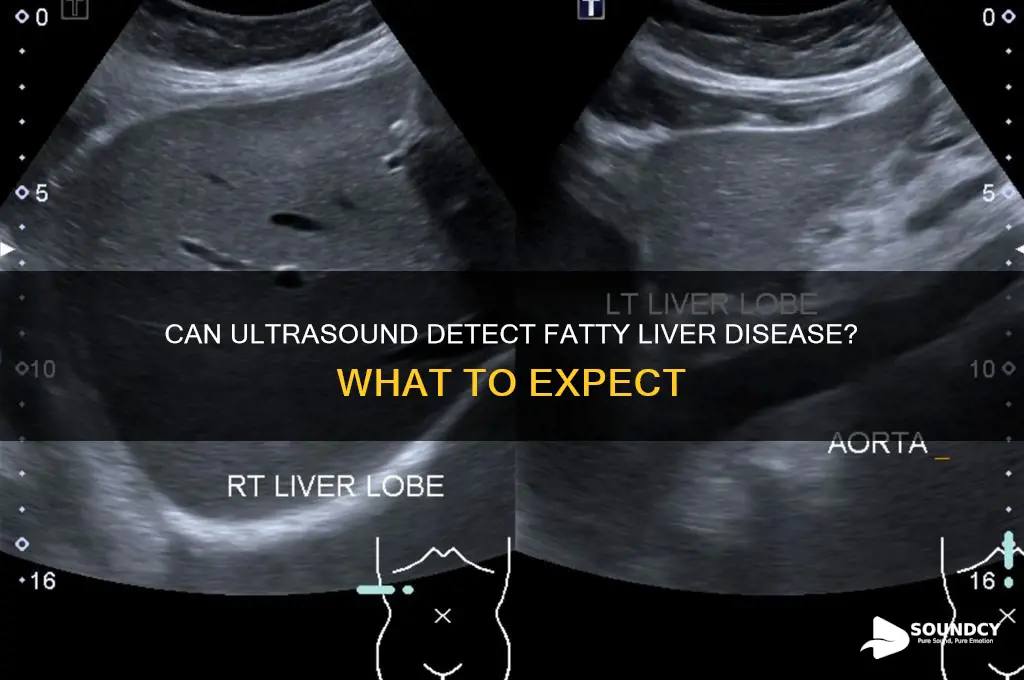
Fatty liver, a condition characterized by the accumulation of excess fat in liver cells, is a growing concern due to its association with obesity, diabetes, and metabolic syndrome. One of the most common diagnostic tools used to detect fatty liver is an ultrasound, which is non-invasive, widely available, and cost-effective. During an ultrasound, high-frequency sound waves create images of the liver, allowing healthcare providers to assess its size, texture, and echogenicity. Fatty liver typically appears as a brighter (hyperechoic) liver compared to the kidneys, a key indicator of fat infiltration. While ultrasound is highly effective in identifying moderate to severe cases, it may not always detect mild fatty liver or differentiate between simple fatty liver and more advanced conditions like non-alcoholic steatohepatitis (NASH). Therefore, while ultrasound is a valuable initial screening tool, additional tests such as blood work, elastography, or imaging modalities like MRI or CT scans may be necessary for a comprehensive diagnosis.
| Characteristics | Values |
|---|---|
| Detection Method | Ultrasound is a common imaging technique used to detect fatty liver disease (FLD). |
| Appearance on Ultrasound | Fatty liver typically appears as a diffusely increased echogenicity (brightness) of the liver parenchyma compared to the kidneys and spleen. |
| Sensitivity | Ultrasound has a sensitivity of approximately 85-90% for detecting moderate to severe fatty liver disease. |
| Specificity | Specificity is around 90-95% for diagnosing fatty liver, but it may not differentiate between simple fatty liver and more advanced stages like steatohepatitis. |
| Limitations | Ultrasound may not detect mild fatty infiltration (<30% fat) and cannot quantify the exact amount of fat in the liver. It also cannot diagnose the severity of liver fibrosis or cirrhosis. |
| Advantages | Non-invasive, widely available, cost-effective, and does not use ionizing radiation. |
| Confirmation | Further tests like MRI, CT scan, or liver biopsy may be needed for confirmation, especially in cases of suspected advanced liver disease. |
| Associated Findings | Ultrasound may reveal hepatomegaly (enlarged liver) and signs of portal hypertension in advanced cases. |
| Grading | Ultrasound can provide a semi-quantitative assessment of fatty liver severity based on echogenicity and visibility of vascular structures. |
| Latest Research | Advances in ultrasound techniques, such as shear wave elastography, can help assess liver stiffness and fibrosis, improving diagnostic accuracy. |
Explore related products


$13 $19.99

$109.99 $129.99



What You'll Learn
![]()
Ultrasound accuracy for fatty liver detection
Ultrasound imaging has become a cornerstone in the non-invasive assessment of fatty liver disease (FLD), offering a radiation-free and cost-effective alternative to more invasive procedures. Its accuracy in detecting hepatic steatosis—the accumulation of fat in the liver—is well-documented, with studies showing sensitivity and specificity rates ranging from 80% to 95% when compared to biopsy, the gold standard. However, these figures are contingent on the severity of fat infiltration; ultrasound is most reliable in cases of moderate to severe fatty liver, where fat comprises over 30% of liver volume. Mild cases, particularly those with less than 20% fat, may elude detection due to subtle changes in echogenicity, the brightness of the liver tissue on the scan.
To maximize accuracy, technicians must adhere to specific protocols during the examination. Patients are typically instructed to fast for at least 6 hours prior to the scan, as recent food intake can artificially elevate liver echogenicity, mimicking fat deposition. The use of high-frequency transducers (3.5–5 MHz) and standardized imaging planes, such as the right upper quadrant in the midclavicular line, further enhances diagnostic precision. Radiologists also assess for ancillary signs, like liver-to-kidney contrast and posterior beam attenuation, which bolster confidence in the diagnosis. Despite these measures, interobserver variability remains a challenge, underscoring the need for experienced operators.
While ultrasound excels in detecting fatty liver, it falls short in grading fibrosis or inflammation, key components of non-alcoholic steatohepatitis (NASH). This limitation necessitates complementary tools like elastography or serum biomarkers for comprehensive evaluation. For instance, shear wave elastography, often integrated with ultrasound systems, quantifies liver stiffness, correlating with fibrosis stage. Combining these modalities can improve diagnostic yield, particularly in patients at risk for disease progression, such as those with metabolic syndrome or obesity.
In clinical practice, ultrasound serves as a first-line screening tool for FLD, especially in asymptomatic individuals with risk factors like diabetes or hyperlipidemia. Its accessibility and safety profile make it ideal for longitudinal monitoring, enabling early intervention through lifestyle modifications or pharmacotherapy. However, false negatives can occur in early-stage disease or in patients with certain body habitus, such as severe obesity or narrow intercostal spaces, which impede sound wave penetration. In such cases, alternative imaging modalities like MRI or CT may be warranted.
Ultimately, the accuracy of ultrasound for fatty liver detection hinges on technical proficiency, patient preparation, and disease severity. While it is not infallible, its role in identifying at-risk individuals and guiding management is invaluable. Clinicians must interpret results within the clinical context, recognizing both the strengths and limitations of this imaging modality. For patients, understanding that ultrasound provides a snapshot of liver health—not a complete picture—is essential for informed decision-making.
Exploring the Mystical Sound Frequency of 432Hz: Harmony and Healing
You may want to see also
Explore related products





![]()
Appearance of fatty liver on ultrasound
Fatty liver, or hepatic steatosis, presents distinct characteristics on ultrasound that radiologists and clinicians use to diagnose this condition. The liver appears diffusely echogenic, meaning it reflects more sound waves and looks brighter than the kidneys or spleen, which are normally of similar echogenicity. This increased brightness is a hallmark of fat accumulation within hepatocytes, often described as a "bright liver" on imaging reports. The echogenicity is typically uniform, though in advanced cases, the liver’s edges may appear slightly blurred due to fat infiltration.
One key feature to note is the posterior beam attenuation, where the ultrasound beam weakens as it passes through fatty tissue. This results in poor visualization of deeper structures, such as the diaphragm or abdominal organs behind the liver. Additionally, the blood vessels within the liver, particularly the portal veins and hepatic veins, may appear more prominent against the bright background, a phenomenon known as "vascular sparing." These vascular structures stand out as darker lines in contrast to the echogenic parenchyma.
Comparing fatty liver to other conditions is crucial for accurate diagnosis. For instance, cirrhosis may also cause a bright liver, but it is often accompanied by nodularity and irregular liver contours, unlike the smooth appearance of fatty liver. Hemangiomas or tumors present as focal lesions, whereas fatty liver is diffuse. Ultrasound alone cannot quantify the degree of fat accumulation, but it provides a reliable initial assessment, often prompting further evaluation with elastography or biopsy.
Practical tips for interpreting ultrasound findings include ensuring proper patient preparation, such as fasting for at least 6 hours, as recent food intake can mimic fatty changes. Radiologists should also correlate ultrasound findings with clinical history, such as obesity, diabetes, or metabolic syndrome, which are common risk factors. While ultrasound is highly sensitive for detecting moderate to severe fatty liver, mild cases may be missed, especially in early stages. Thus, it serves as a screening tool rather than a definitive diagnostic method.
In conclusion, the appearance of fatty liver on ultrasound is characterized by diffuse increased echogenicity, posterior beam attenuation, and vascular sparing. Recognizing these features is essential for early detection and management, particularly in high-risk populations. While ultrasound is invaluable for initial assessment, it should be complemented by additional imaging or laboratory tests to confirm the diagnosis and assess disease severity.
What Does a Blown Speaker Sound Like? Identifying the Distorted Audio
You may want to see also
Explore related products






![]()
Limitations of ultrasound in diagnosis
Ultrasound is a widely used imaging tool for detecting fatty liver disease, but it’s not without its limitations. One major constraint is its inability to quantify the degree of fat accumulation accurately. While ultrasound can identify moderate to severe fatty liver, it struggles with mild cases, often missing early-stage disease. This limitation arises because subtle changes in liver echogenicity—the brightness of the liver on the scan—can be difficult to distinguish from normal variations. For instance, a mildly fatty liver may appear only slightly brighter than a healthy liver, leading to potential false negatives. Clinicians must therefore interpret results cautiously, especially when screening patients at risk but without overt symptoms.
Another critical limitation is ultrasound’s reliance on operator skill and machine quality. The accuracy of the scan depends heavily on the technician’s expertise in positioning the probe and adjusting settings like depth and gain. Inconsistent technique can lead to variability in results, making it harder to compare scans over time or across different facilities. For example, a poorly performed ultrasound might overestimate fat content due to excessive gain, while a suboptimal probe angle could obscure key areas of the liver. Standardizing protocols and ensuring technician training are essential to mitigate these issues, but they remain inherent challenges in ultrasound-based diagnosis.
Ultrasound also falls short in differentiating between simple fatty liver and more advanced conditions like steatohepatitis or cirrhosis. While it can detect liver enlargement or nodularity, it cannot assess cellular-level damage or fibrosis. This limitation often necessitates additional tests, such as elastography or biopsy, to determine disease severity. For instance, a patient with a fatty liver on ultrasound might require a FibroScan to measure liver stiffness, adding time and cost to the diagnostic process. Ultrasound’s inability to provide a comprehensive assessment underscores its role as a screening tool rather than a definitive diagnostic method.
Lastly, certain patient factors can compromise ultrasound’s effectiveness. Obesity, for example, reduces sound wave penetration, leading to poor image quality and potential misdiagnosis. Similarly, patients with excessive bowel gas or those who cannot hold their breath adequately during the scan may yield suboptimal results. In such cases, alternative imaging modalities like MRI or CT may be more reliable, though they come with their own drawbacks, such as higher cost and radiation exposure. Understanding these limitations helps clinicians tailor their approach, ensuring that ultrasound is used appropriately within its diagnostic scope.
Do Alarms Sound on FaceTime? Exploring Notifications During Calls
You may want to see also
Explore related products





![]()
Differentiating fatty liver from other conditions
Fatty liver disease, characterized by excessive fat accumulation in the liver, often presents unique challenges in diagnosis due to its overlap with other hepatic conditions. Ultrasound imaging, a common diagnostic tool, can detect fatty liver by revealing increased echogenicity of the liver compared to the kidneys. However, this finding is not exclusive to fatty liver disease, as conditions like cirrhosis, hepatitis, and liver tumors can also alter liver echogenicity. Differentiating fatty liver from these conditions requires a nuanced approach, combining imaging findings with clinical context and additional tests.
For instance, while fatty liver typically shows diffuse echogenicity without focal lesions, liver tumors often present as distinct masses. Cirrhosis, on the other hand, may exhibit a nodular liver surface and splenomegaly, features not commonly seen in early-stage fatty liver. Ultrasound alone cannot definitively distinguish these conditions, but it serves as a critical first step. Follow-up with elastography (e.g., FibroScan) or MRI can assess liver stiffness and fat content, aiding in differentiation. For example, a FibroScan score above 7.5 kPa suggests advanced fibrosis, more indicative of cirrhosis than fatty liver.
Clinicians must also consider patient history and risk factors. Fatty liver is strongly associated with obesity, diabetes, and metabolic syndrome, whereas viral hepatitis or alcohol abuse may point to other liver diseases. Laboratory tests, such as elevated ALT and AST levels, are common in both fatty liver and hepatitis but can be further clarified with viral serology or ferritin levels to rule out hemochromatosis. For patients over 40 with unexplained weight loss, a workup for liver cancer should be prioritized, even if ultrasound findings initially suggest fatty liver.
In practice, a systematic approach is key. Start with ultrasound to identify echogenicity, then correlate with clinical and lab data. If uncertainty persists, advanced imaging or biopsy may be necessary. For example, a 50-year-old patient with obesity and elevated liver enzymes but no history of alcohol use is more likely to have fatty liver than cirrhosis, but confirmation with elastography ensures accuracy. This stepwise strategy minimizes misdiagnosis and guides appropriate management, whether lifestyle modifications for fatty liver or antiviral therapy for hepatitis.
Ultimately, differentiating fatty liver from other conditions requires integrating ultrasound findings with clinical judgment and ancillary tests. While ultrasound is a valuable initial tool, its limitations underscore the importance of a comprehensive diagnostic approach. By combining imaging, patient history, and laboratory data, clinicians can accurately identify fatty liver and tailor interventions to address the underlying cause, improving patient outcomes and preventing disease progression.
East End vs. Australian Accent: Unraveling the Similarities and Differences
You may want to see also
Explore related products





![]()
When additional imaging is needed
Ultrasound is often the first imaging test used to detect fatty liver disease due to its non-invasive nature and accessibility. However, it has limitations in quantifying fat content and distinguishing between simple fatty liver and more severe conditions like steatohepatitis or cirrhosis. When ultrasound findings are inconclusive or further detail is required, additional imaging modalities become necessary. For instance, a patient with suspected fatty liver and elevated liver enzymes may need more advanced imaging to assess the extent of liver damage and guide treatment decisions.
Steps to Determine the Need for Additional Imaging:
- Evaluate Ultrasound Results: If the ultrasound shows moderate to severe fatty infiltration but lacks clarity on liver texture or nodularity, consider further imaging.
- Assess Symptoms and Risk Factors: Patients with persistent symptoms (e.g., fatigue, abdominal pain) or risk factors (e.g., obesity, diabetes) may require more detailed evaluation.
- Consult Laboratory Tests: Elevated liver enzymes (ALT, AST) or markers of fibrosis (e.g., FIB-4 score) can indicate the need for advanced imaging to rule out progression to fibrosis or cirrhosis.
Cautions in Relying Solely on Ultrasound:
Ultrasound’s accuracy decreases in obese patients or those with significant bowel gas, which can obscure liver visualization. Additionally, it cannot differentiate between steatosis (simple fatty liver) and steatohepatitis (inflammation and fat), a critical distinction for treatment planning. For example, a patient with non-alcoholic fatty liver disease (NAFLD) may appear similar on ultrasound to one with non-alcoholic steatohepatitis (NASH), but the latter requires aggressive management to prevent cirrhosis.
Advanced Imaging Options:
Practical Tips for Patients:
If your doctor recommends additional imaging, ask about the specific modality and its purpose. For MRI-PDFF, avoid eating or drinking for 4 hours prior to the scan. For FibroScan, wear loose clothing and lie still during the procedure. Understanding the rationale behind the imaging can reduce anxiety and ensure compliance with preparation instructions.
In summary, while ultrasound is a valuable initial tool for detecting fatty liver, its limitations often necessitate additional imaging to refine diagnosis and guide treatment. Advanced modalities like MRI-PDFF and FibroScan provide critical insights into fat quantification and fibrosis staging, ensuring patients receive targeted care tailored to their condition.
Do American Buffalo Make Sounds? Exploring Their Unique Vocalizations
You may want to see also
Frequently asked questions
Fatty liver is usually detectable on an ultrasound, but the accuracy depends on the severity of the condition. Mild cases may be harder to identify, while moderate to severe fatty liver is typically visible.
An ultrasound can indicate the presence of fatty liver but cannot distinguish between simple fatty liver (steatosis) and non-alcoholic steatohepatitis (NASH). Further tests like a biopsy or blood work may be needed for a definitive diagnosis.
Yes, ultrasound has limitations. It may not detect early-stage fatty liver, and its accuracy can be affected by factors like obesity, bowel gas, or the patient's body habitus. Additional imaging or tests may be required for confirmation.































