Transvaginal ultrasound (TVUS) is a valuable diagnostic tool commonly used to assess the female pelvic organs, including the uterus and endometrium. When investigating potential signs of endometrial cancer, TVUS plays a crucial role by providing detailed images of the endometrial lining, allowing healthcare providers to detect abnormalities such as thickening, irregular contours, or the presence of masses. While TVUS can identify suspicious findings that may suggest endometrial cancer, it is not definitive for diagnosis. Further evaluation, such as endometrial biopsy or hysteroscopy, is often necessary to confirm the presence of cancer. Nonetheless, TVUS remains an essential first-line imaging modality for early detection and monitoring of endometrial abnormalities that could indicate malignancy.
| Characteristics | Values |
|---|---|
| Detection of Endometrial Thickness | A transvaginal ultrasound (TVUS) measures endometrial thickness, which is a key indicator. A thickness >4 mm postmenopausal or >15 mm premenopausal may suggest endometrial cancer, but it is not diagnostic alone. |
| Endometrial Appearance | Abnormalities like irregular echogenicity, focal lesions, or cystic areas may indicate cancer, but findings are not specific and require further evaluation. |
| Diagnostic Accuracy | TVUS has moderate sensitivity (60-80%) and specificity (70-90%) for detecting endometrial cancer. It is a useful initial screening tool but not definitive. |
| Limitations | Cannot differentiate between benign and malignant lesions. False positives and negatives are common, especially in cases of endometrial hyperplasia or polyps. |
| Follow-Up Required | Abnormal findings necessitate further tests like endometrial biopsy, hysteroscopy, or MRI for confirmation. |
| Role in Staging | Limited role in staging endometrial cancer; advanced imaging like CT or MRI is preferred for assessing spread. |
| Patient Population | Most effective in postmenopausal women or those with abnormal uterine bleeding (AUB). Less reliable in premenopausal women due to cyclical changes. |
| Operator Dependency | Accuracy depends on technician skill and image interpretation, which can vary. |
| Cost-Effectiveness | Relatively low-cost and non-invasive, making it a first-line imaging modality for initial assessment. |
| Latest Guidelines | Recommended by organizations like the American College of Obstetricians and Gynecologists (ACOG) for evaluating AUB and endometrial abnormalities. |
Explore related products






What You'll Learn
![]()
Accuracy of transvaginal ultrasound in detecting endometrial cancer
Transvaginal ultrasound (TVUS) is a cornerstone in the evaluation of endometrial abnormalities, offering a non-invasive method to visualize the endometrial lining. Its accuracy in detecting endometrial cancer hinges on several factors, including the skill of the sonographer, the quality of the equipment, and the patient’s clinical context. Studies consistently show that TVUS can reliably measure endometrial thickness, a key indicator of potential malignancy. For postmenopausal women, an endometrial thickness greater than 4–5 mm warrants further investigation, as it may suggest hyperplasia or cancer. However, thickness alone is not diagnostic; TVUS also assesses endometrial echogenicity, morphology, and the presence of focal lesions, which enhance its predictive value.
One of the strengths of TVUS lies in its ability to differentiate between benign and malignant conditions. For instance, a heterogeneous endometrium or the presence of a focal mass raises suspicion for cancer. However, its accuracy is not absolute. False positives can occur in cases of endometrial polyps or hyperplasia without atypia, while false negatives may arise in early-stage cancers with minimal endometrial changes. A meta-analysis published in the *Journal of Ultrasound in Medicine* reported a sensitivity of 86% and specificity of 89% for TVUS in detecting endometrial cancer, underscoring its utility while highlighting its limitations.
To maximize the accuracy of TVUS, clinicians should integrate it with other diagnostic tools. For example, combining TVUS with endometrial biopsy or saline infusion sonography (SIS) can improve detection rates, particularly in cases where the endometrium appears normal or ambiguous. SIS, in particular, enhances visualization by distending the uterine cavity, making it easier to identify subtle abnormalities. Additionally, patient preparation, such as ensuring the bladder is partially full, optimizes image quality and diagnostic yield.
Despite its effectiveness, TVUS is not a standalone test for endometrial cancer. Its role is primarily to triage patients for further evaluation, such as biopsy or hysteroscopy. For high-risk individuals, including those with persistent abnormal uterine bleeding or a history of estrogen-only hormone therapy, TVUS serves as an initial screening tool. However, reliance on TVUS alone can lead to missed diagnoses, particularly in cancers confined to the myometrium or those with minimal endometrial involvement. Thus, clinical judgment and a comprehensive approach remain paramount.
In practice, understanding the nuances of TVUS interpretation is critical. For instance, a thickened endometrium in a premenopausal woman may be physiological, especially during the secretory phase of the menstrual cycle, whereas the same finding in a postmenopausal woman is highly concerning. Radiologists and gynecologists must correlate ultrasound findings with patient history, symptoms, and risk factors to avoid misinterpretation. By doing so, TVUS becomes a powerful tool in the early detection and management of endometrial cancer, balancing accuracy with the need for additional diagnostic steps.
Unveiling the Unique Vocalizations: What Sounds Do Geckos Make?
You may want to see also
Explore related products






![]()
Common ultrasound findings suggestive of endometrial cancer
Transvaginal ultrasound (TVUS) is a frontline imaging tool for evaluating the endometrium, offering detailed visualization of the uterine lining and surrounding structures. While it cannot definitively diagnose endometrial cancer, certain findings strongly suggest the presence of malignancy. One of the most critical indicators is an endometrial thickness exceeding 4–5 mm in postmenopausal women or those not on hormone replacement therapy. This measurement, however, is not absolute; younger premenopausal women may naturally have thicker endometria, necessitating correlation with clinical symptoms and risk factors.
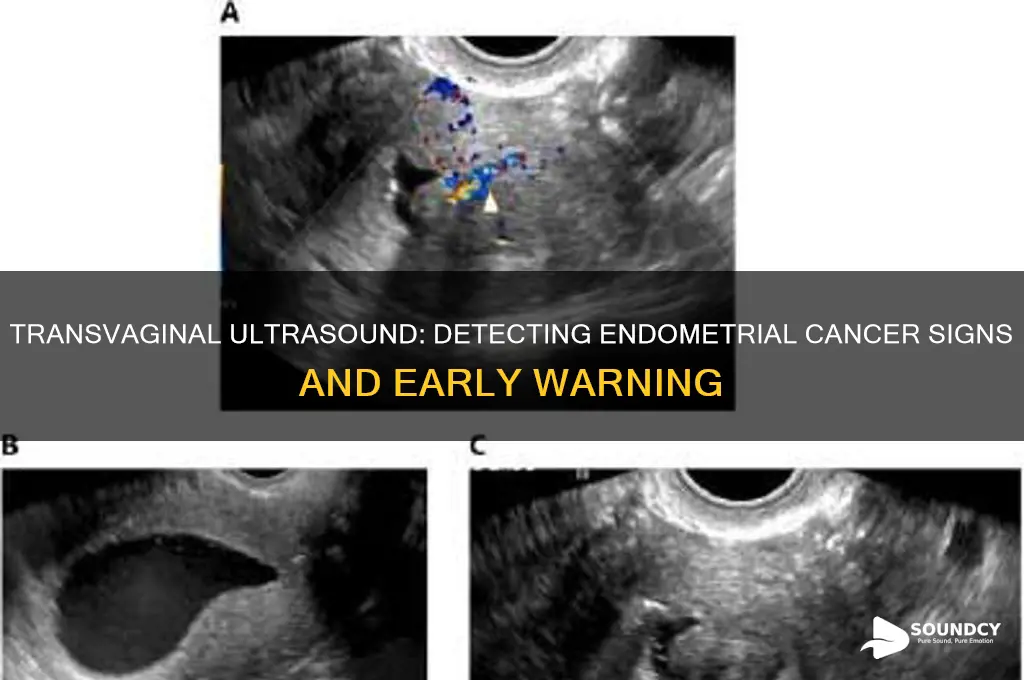
Beyond thickness, the morphology of the endometrial stripe provides valuable clues. A heterogeneous or irregular appearance, particularly with cystic spaces or focal masses, raises suspicion. These abnormalities often reflect hyperplasia or invasive carcinoma, disrupting the normal trilaminar pattern seen in healthy endometria. Color Doppler assessment may further enhance diagnostic accuracy by revealing increased vascularity within the endometrium, a feature commonly associated with malignancy.
Another red flag is the presence of a focal endometrial lesion, which may appear as a discrete mass or polypoid structure. Such lesions often demonstrate irregular borders, internal vascularity, and posterior shadowing, distinguishing them from benign polyps. In advanced cases, myometrial invasion may be evident, characterized by disruption of the junctional zone or extension into the outer myometrium, a finding that correlates with higher-grade tumors and poorer prognosis.
While TVUS is highly sensitive for detecting endometrial abnormalities, its specificity is limited. False positives can arise from conditions like hyperplasia, polyps, or atrophic endometrium, while false negatives may occur in cases of small, early-stage cancers. Therefore, abnormal findings should prompt further evaluation, such as endometrial biopsy or hysteroscopy, to confirm the diagnosis. Combining clinical history, risk factors, and imaging results ensures a comprehensive approach to identifying endometrial cancer.
Unraveling the Mystery: What Causes That Mysterious Booming Sound?
You may want to see also
Explore related products




![]()
Limitations of transvaginal ultrasound in cancer diagnosis
Transvaginal ultrasound (TVUS) is a valuable tool in gynecological assessments, often used to evaluate the endometrium for abnormalities, including potential signs of endometrial cancer. However, its effectiveness is not without boundaries. One significant limitation lies in its inability to definitively diagnose cancer. TVUS can detect endometrial thickening, a potential indicator of malignancy, but it cannot distinguish between benign conditions like hyperplasia and cancerous lesions. For instance, a postmenopausal woman with an endometrial thickness exceeding 4 mm may prompt concern, but biopsy remains the gold standard for confirmation.
Another constraint arises from operator dependency and anatomical variations. The accuracy of TVUS relies heavily on the skill and experience of the sonographer. Subtle abnormalities, such as small focal lesions or early-stage cancers, may be overlooked if not meticulously examined. Additionally, factors like obesity, uterine position, or the presence of fibroids can obscure visualization, reducing diagnostic reliability. For example, a tilted uterus or dense fibroid tissue might mimic endometrial thickening, leading to false positives or negatives.
While TVUS provides real-time imaging and is non-invasive, it lacks the tissue characterization capabilities of more advanced modalities like MRI or biopsy. It cannot assess cellular changes or determine the depth of myometrial invasion, both critical factors in staging endometrial cancer. For instance, a TVUS may show a thickened endometrium but cannot reveal whether the cancer has penetrated beyond 50% of the myometrium, a key determinant for surgical planning and prognosis.
Lastly, TVUS is less effective in detecting early-stage or minimally invasive cancers, which may not present with significant endometrial thickening. These cases often require more sensitive techniques, such as hysteroscopy or endometrial sampling, to identify microscopic abnormalities. For women at high risk, such as those with Lynch syndrome or a history of tamoxifen use, relying solely on TVUS could delay diagnosis and treatment. Thus, while TVUS is a useful initial screening tool, its limitations underscore the need for complementary diagnostic approaches in evaluating endometrial cancer.
How CDs Produce Sound: Unraveling the Magic of Laser Technology
You may want to see also
Explore related products






![]()
Role of ultrasound in endometrial cancer screening
Transvaginal ultrasound (TVUS) plays a pivotal role in the early detection and evaluation of endometrial cancer, particularly in postmenopausal women or those with abnormal uterine bleeding. By measuring endometrial thickness, TVUS serves as a non-invasive, cost-effective tool to identify high-risk individuals who may require further diagnostic workup. Studies indicate that an endometrial thickness of greater than 4 mm in postmenopausal women or 15 mm in premenopausal women warrants additional investigation, such as biopsy or hysteroscopy. This threshold-based approach helps stratify risk while minimizing unnecessary procedures.
However, TVUS is not without limitations. While it can suggest abnormalities, it cannot definitively diagnose endometrial cancer. Its accuracy depends on factors like operator skill, patient anatomy, and the presence of conditions such as endometrial hyperplasia or polyps, which may mimic cancer. For instance, a thickened endometrium could result from hormonal imbalances rather than malignancy. Therefore, TVUS acts as a screening tool, guiding clinicians to pursue more definitive tests when suspicious findings arise.
Incorporating TVUS into routine screening protocols requires careful consideration of patient demographics and risk factors. For asymptomatic women, routine screening is generally not recommended unless they have a high-risk profile, such as a history of unopposed estrogen therapy or hereditary cancer syndromes like Lynch syndrome. In contrast, symptomatic patients, particularly those with postmenopausal bleeding, benefit significantly from TVUS as an initial diagnostic step. Practical tips include ensuring adequate bladder emptying for better visualization and using color Doppler to assess vascularity, which may enhance detection of malignant lesions.
Comparatively, TVUS offers advantages over other imaging modalities like MRI or CT in endometrial cancer screening due to its accessibility, lower cost, and lack of radiation exposure. However, MRI provides superior soft-tissue contrast and is often used for staging once cancer is confirmed. The choice of imaging depends on clinical context, with TVUS serving as the first-line option for initial assessment. By understanding its role and limitations, clinicians can effectively integrate TVUS into a tiered diagnostic approach, optimizing early detection while minimizing overdiagnosis.
Are Beats Headphones Worth the Hype for Sound Quality?
You may want to see also
Explore related products






![]()
Need for additional tests after abnormal ultrasound results
Abnormal results from a transvaginal ultrasound can be alarming, particularly when evaluating for endometrial cancer. While this imaging technique provides valuable insights into the thickness and appearance of the endometrium, it is not definitive. An endometrial lining thicker than 4 mm postmenopause or irregular in premenopausal women may raise suspicion, but these findings alone are insufficient for diagnosis. The ultrasound serves as a screening tool, flagging potential issues that necessitate further investigation to confirm or rule out malignancy.
Once an abnormality is detected, the next step typically involves endometrial biopsy, the gold standard for diagnosing endometrial cancer. This procedure, often performed in an outpatient setting, collects tissue samples for pathological examination. For postmenopausal women with a lining thickness between 4–10 mm, a biopsy is recommended, while those above 10 mm require immediate evaluation. Premenopausal women with abnormal bleeding or persistent ultrasound findings should also undergo biopsy, regardless of lining thickness. This targeted approach ensures that suspicious cases are not overlooked.
In some instances, additional imaging modalities may complement the initial ultrasound. MRI, for example, offers detailed visualization of the pelvic anatomy, helping differentiate between benign conditions like polyps or hyperplasia and malignant tumors. Hysteroscopy, a minimally invasive procedure using a thin, lighted scope, allows direct visualization of the uterine cavity and can guide biopsy or polyp removal. These tools provide a more comprehensive assessment, particularly in complex cases where ultrasound findings are inconclusive.
While further testing is crucial, it’s essential to balance diagnostic accuracy with patient anxiety and procedural risks. Biopsies, though generally safe, carry a small risk of infection or bleeding, and repeated procedures can be distressing. Clinicians must weigh the benefits of additional tests against the potential harm, especially in low-risk cases. Shared decision-making, involving patients in the discussion of next steps, ensures that their concerns and preferences are addressed while pursuing a definitive diagnosis.
Ultimately, an abnormal transvaginal ultrasound is a call to action, not a verdict. It prompts a structured approach to rule out endometrial cancer through biopsies, advanced imaging, or direct visualization. Each step is tailored to the patient’s risk profile, ensuring timely and accurate diagnosis while minimizing unnecessary interventions. This layered strategy underscores the importance of not relying solely on ultrasound results but using them as a foundation for further exploration.
The Symphony Within: Decoding the Unique Sounds of a Heart
You may want to see also
Frequently asked questions
No, a transvaginal ultrasound cannot definitively diagnose endometrial cancer. It can detect abnormalities in the endometrial lining, such as thickening or masses, but a biopsy is needed for a confirmed diagnosis.
A transvaginal ultrasound may show an abnormally thickened endometrial lining, irregular shapes or masses within the uterus, or fluid in the endometrial cavity, which could suggest endometrial cancer.
Not always. A normal ultrasound does not completely rule out endometrial cancer, as some early-stage cancers or small lesions may not be visible. Further evaluation may be necessary if symptoms persist.
Yes, a transvaginal ultrasound is often the first imaging test used to evaluate the endometrium when endometrial cancer is suspected, especially in women with abnormal bleeding or other risk factors.
If the ultrasound shows abnormalities, a biopsy (such as an endometrial biopsy or dilation and curettage) is typically performed to confirm the diagnosis and determine the presence of cancerous cells.
























