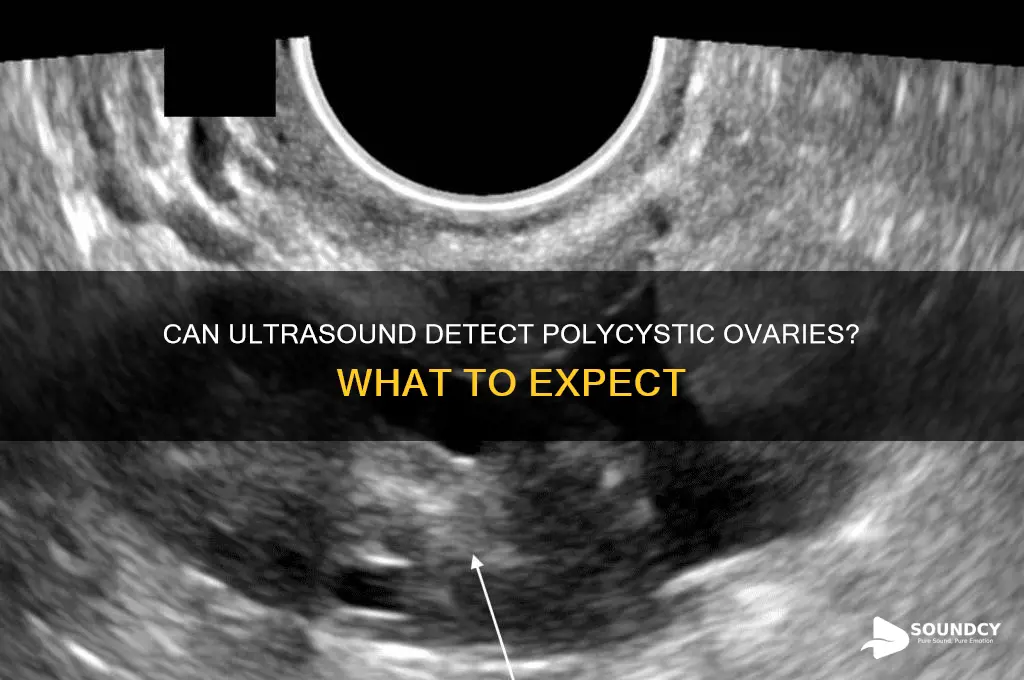
Polycystic ovaries, a hallmark of Polycystic Ovary Syndrome (PCOS), are often detected through transvaginal or transabdominal ultrasound imaging. During an ultrasound, the technician examines the ovaries for the presence of multiple small follicles, typically measuring 2-9 mm in diameter, which are arranged peripherally in a string of pearls pattern. This characteristic appearance, along with an enlarged ovarian volume, is a key diagnostic criterion for polycystic ovaries. Ultrasound is a non-invasive and highly effective tool for visualizing these abnormalities, making it a crucial component in the evaluation and diagnosis of PCOS. However, it’s important to note that not all women with PCOS will exhibit polycystic ovaries on ultrasound, as the condition is diagnosed based on a combination of clinical, hormonal, and imaging findings.
| Characteristics | Values |
|---|---|
| Visibility on Ultrasound | Yes, polycystic ovaries (PCO) are typically visible on transvaginal or transabdominal ultrasound. |
| Key Ultrasound Findings | 1. Enlarged Ovaries: Volume ≥10 mL (most common criterion). 2. Follicle Count: 12 or more follicles measuring 2–9 mm in diameter per ovary. 3. Peripheral Follicle Distribution: Follicles clustered around the ovarian periphery. |
| Diagnostic Criteria (Rotterdam) | Ultrasound criteria alone are insufficient; diagnosis requires 2 out of 3: 1. Ultrasound findings. 2. Oligo/anovulation. 3. Hyperandrogenism (clinical or biochemical). |
| Sensitivity of Ultrasound | High, especially for detecting enlarged ovaries and follicular abnormalities. |
| Limitations | Cannot diagnose PCOS solely; clinical correlation needed. May miss mild cases or overlap with normal variants. |
| Additional Imaging Features | Stromal echogenicity may be increased, but not always present. |
| Differential Diagnosis | Distinguish from physiological follicular growth, premature ovarian insufficiency, or other ovarian conditions. |
| Gold Standard Confirmation | Clinical assessment + ultrasound + hormonal evaluation (e.g., LH/FSH ratio, testosterone levels). |
| Latest Guidelines (2023) | Emphasize ovarian volume ≥10 mL and follicle count ≥12 as primary ultrasound markers. |
| False Positives/Negatives | Possible false positives in perimenopausal women or false negatives in lean PCOS patients with less pronounced ovarian changes. |
Explore related products






What You'll Learn
![]()
Ultrasound accuracy for PCOS detection
Polycystic ovary syndrome (PCOS) is a complex condition, and ultrasound plays a pivotal role in its diagnosis. However, the accuracy of ultrasound for detecting PCOS is not absolute and depends on several factors, including the skill of the sonographer, the quality of the equipment, and the specific criteria used to interpret the images. According to the Rotterdam criteria, one of the diagnostic pillars for PCOS is the presence of 12 or more follicles measuring 2–9 mm in diameter in one or both ovaries, or an ovarian volume greater than 10 mL. These features are typically visible on transvaginal ultrasound, which is more sensitive than transabdominal ultrasound for this purpose.
To maximize accuracy, it’s essential to follow specific protocols during the ultrasound examination. The scan should be performed during the early follicular phase of the menstrual cycle (days 2–5) to avoid misinterpretation of developing follicles. The sonographer must carefully measure ovarian volume and follicle count, ensuring consistency in technique. For instance, using a 3D ultrasound can provide more precise volume measurements compared to 2D imaging, though it is not always necessary. Patients should be informed to avoid pelvic exams or intercourse 24–48 hours before the scan, as these can alter follicle appearance.
Despite its utility, ultrasound has limitations in PCOS detection. One challenge is the subjective interpretation of follicle count and ovarian morphology. Studies show interobserver variability, meaning different sonographers may report varying findings for the same patient. Additionally, up to 20% of women without PCOS may have polycystic-appearing ovaries on ultrasound, leading to potential false positives. Conversely, some women with PCOS may not meet the follicle count or volume criteria, particularly if they are postmenopausal or have undergone ovarian surgery.
Comparatively, ultrasound remains the most accessible and non-invasive imaging tool for PCOS diagnosis, especially when combined with clinical and hormonal assessments. While MRI or CT scans can provide more detailed images, they are costly and unnecessary for routine PCOS evaluation. For optimal results, ultrasound should be part of a multidisciplinary approach, including hormonal tests (e.g., elevated androgens) and symptom evaluation (e.g., irregular periods, hirsutism). Patients should be aware that a single ultrasound may not provide a definitive diagnosis, and repeat scans or additional tests may be required.
In conclusion, ultrasound is a valuable but not infallible tool for detecting PCOS. Its accuracy hinges on proper technique, timing, and interpretation. Patients and healthcare providers should approach ultrasound findings as one piece of the diagnostic puzzle, ensuring a comprehensive evaluation to avoid misdiagnosis. For those undergoing PCOS assessment, understanding these nuances can foster informed discussions with their healthcare team and more accurate management plans.
How Sweet the Sound: 25 Unforgettable FA Moments in Music
You may want to see also
Explore related products






![]()
Transvaginal vs. transabdominal ultrasound
Polycystic ovaries (PCO) are typically diagnosed through ultrasound, but the choice between transvaginal and transabdominal ultrasound can significantly impact the accuracy and clarity of the results. Transvaginal ultrasound involves inserting a probe into the vagina to obtain images of the pelvic organs, while transabdominal ultrasound uses a probe moved across the abdomen to capture images. Both methods have distinct advantages and limitations when it comes to detecting PCO.
From an analytical perspective, transvaginal ultrasound is generally considered superior for evaluating ovarian morphology due to its higher resolution and proximity to the ovaries. It allows for better visualization of small follicles (typically 2–9 mm in diameter) and the ovarian stroma, which are critical for diagnosing PCO. The transvaginal approach is particularly useful in younger patients or those with a higher body mass index (BMI), where abdominal fat can obscure transabdominal images. However, it may be less comfortable or culturally acceptable for some individuals, which can influence patient preference.
Instructively, if you are undergoing an ultrasound for PCO, here’s what to expect: For a transvaginal ultrasound, you’ll be asked to empty your bladder and lie on your back, while a lubricated probe is gently inserted into the vagina. The procedure typically takes 10–15 minutes and is minimally invasive. For a transabdominal ultrasound, you’ll need a full bladder to help visualize the pelvic organs, so drink 1–1.5 liters of water an hour before the exam. The probe will be moved across your lower abdomen with gel to improve image quality. Both procedures are safe and do not involve radiation.
Comparatively, while transabdominal ultrasound is non-invasive and often the first choice for initial pelvic imaging, it may miss subtle PCO features due to its lower resolution. For instance, it can struggle to accurately count small follicles or assess stromal echogenicity, which are key diagnostic criteria for PCO. Transvaginal ultrasound, on the other hand, provides clearer images but may not be suitable for all patients, such as virgins or those with pelvic discomfort. In cases where transvaginal ultrasound is not feasible, transabdominal ultrasound can still provide valuable information, though it may require additional tests for confirmation.
Persuasively, if you suspect PCO or are at risk (e.g., irregular periods, hirsutism, or infertility), advocating for a transvaginal ultrasound can improve diagnostic accuracy. While it may feel more invasive, its ability to detect PCO with greater precision outweighs the temporary discomfort for many. However, if you’re uncomfortable with the transvaginal approach, discuss your concerns with your healthcare provider—they may start with a transabdominal scan and proceed as needed. Ultimately, the choice of method should balance diagnostic needs with patient comfort and preferences.
Unraveling the Mysteries of Human Sound Perception: A Comprehensive Guide
You may want to see also
Explore related products




![]()
Follicle count and size criteria
Polycystic ovaries are often identified through ultrasound by evaluating follicle count and size, which are key diagnostic criteria. According to guidelines, an ovary is considered polycystic if it contains 12 or more follicles measuring 2–9 mm in diameter or has an ovarian volume greater than 10 mL. These criteria are part of the Rotterdam diagnostic framework, which requires at least two of three features: polycystic ovarian morphology, hyperandrogenism, or oligo-ovulation/anovulation. Understanding these metrics is crucial for accurate diagnosis, as they differentiate between normal ovarian function and polycystic ovary syndrome (PCOS).
To assess follicle count and size, transvaginal ultrasound is the preferred method due to its higher resolution compared to transabdominal ultrasound. During the scan, follicles are counted and measured in a single plane, typically at the early follicular phase (days 2–5) of the menstrual cycle. It’s important to note that follicle size can vary naturally, but the 2–9 mm range is specifically associated with PCOS. Larger follicles (>9 mm) may indicate ovulation, while smaller ones (<2 mm) are considered primordial or non-growing. Practitioners must avoid overdiagnosis by ensuring measurements are taken consistently and at the appropriate cycle phase.
A common misconception is that all women with polycystic ovaries have PCOS, but this isn’t the case. Up to 20–30% of reproductive-aged women have polycystic ovarian morphology without meeting the full PCOS criteria. This highlights the importance of combining ultrasound findings with clinical symptoms and hormonal assessments. For example, a 25-year-old woman with 15 follicles in one ovary but no hyperandrogenism or menstrual irregularities would not be diagnosed with PCOS based on ultrasound alone.
For those undergoing evaluation, practical tips can improve the accuracy of ultrasound results. Hydration is key, as a full bladder can interfere with transabdominal imaging, while transvaginal scans require an empty bladder. Patients should also track their menstrual cycle to ensure the scan is performed during the early follicular phase. If diagnosed with polycystic ovaries, further tests such as hormone panels (e.g., testosterone, LH/FSH ratio) and metabolic assessments may be recommended to confirm PCOS and guide treatment.
In summary, follicle count and size criteria are essential for identifying polycystic ovaries on ultrasound, but they are just one piece of the diagnostic puzzle. Accurate measurement, proper timing, and integration with clinical data are critical to avoid misdiagnosis. For healthcare providers and patients alike, understanding these specifics ensures a clearer path to managing reproductive health and addressing potential underlying conditions like PCOS.
Is Rockabilly Truly an American Sound? Exploring Its Roots and Influence
You may want to see also
Explore related products





![]()
Ovarian volume measurement
Polycystic ovaries (PCO) are often diagnosed through ultrasound, a key tool in assessing ovarian morphology. One critical aspect of this evaluation is ovarian volume measurement, which provides quantitative data to support the diagnosis of polycystic ovary syndrome (PCOS). Normal ovarian volume typically ranges from 5 to 10 mL in premenopausal women, but in PCOS, the ovaries are often enlarged, exceeding 10 mL. This measurement is obtained by calculating the ovarian dimensions (length, width, and thickness) using the ellipsoid formula: *volume = (length × width × thickness) × 0.523*. Accurate measurement is essential, as an enlarged ovarian volume is one of the Rotterdam criteria for diagnosing PCOS, alongside the presence of 12 or more follicles per ovary and clinical or biochemical signs of hyperandrogenism.
Measuring ovarian volume requires precision and adherence to specific techniques. Transvaginal ultrasound is the preferred method due to its higher resolution compared to transabdominal ultrasound, especially in obese patients or those with enlarged ovaries. The ovary should be visualized in its entirety, and measurements should be taken in the sagittal, coronal, and axial planes to ensure accuracy. It’s crucial to exclude any large cysts or tumors from the measurement, as these can artificially inflate the volume. For consistency, measurements should be performed during the early follicular phase (days 2–5) of the menstrual cycle, as ovarian volume can fluctuate throughout the cycle.
While ovarian volume measurement is a valuable diagnostic tool, it is not without limitations. Interobserver variability can occur due to differences in technique or interpretation, emphasizing the need for standardized training. Additionally, ovarian volume alone is insufficient for a PCOS diagnosis; it must be considered alongside other clinical and ultrasound findings. For instance, a woman with an enlarged ovary but no other PCOS features may not meet diagnostic criteria. Conversely, some women with PCOS may have normal ovarian volumes, particularly in lean phenotypes or early stages of the condition.
In practice, ovarian volume measurement serves as a cornerstone in the ultrasound assessment of PCOS, offering objectivity in a condition often diagnosed through subjective criteria. For healthcare providers, mastering this technique enhances diagnostic accuracy and ensures appropriate patient management. Patients, meanwhile, benefit from understanding that this measurement is part of a broader evaluation, not a standalone test. By integrating ovarian volume measurement with other clinical data, clinicians can provide a more comprehensive and personalized approach to PCOS diagnosis and care.
Understanding Sound Pressure Levels: Newtons in Sound Explained
You may want to see also
Explore related products





![]()
Role of ultrasound in PCOS diagnosis
Ultrasound imaging plays a pivotal role in the diagnosis of Polycystic Ovary Syndrome (PCOS), a complex hormonal disorder affecting women of reproductive age. The characteristic feature of PCOS is the presence of multiple small cysts on the ovaries, which can be visualized through transvaginal or transabdominal ultrasound. These cysts, typically measuring 2-9 mm in diameter, are actually immature follicles that have failed to develop properly due to hormonal imbalances. According to diagnostic criteria, the presence of 12 or more such follicles or an ovarian volume greater than 10 mL in at least one ovary is indicative of PCOS. This imaging technique not only helps in identifying these structural abnormalities but also aids in ruling out other conditions with similar symptoms, such as ovarian tumors or masses.
The procedure for an ultrasound in PCOS diagnosis is straightforward yet requires precision. For a transvaginal ultrasound, the patient is asked to empty her bladder, and a small probe covered with a condom and lubricating gel is inserted into the vagina. This method provides clearer images of the ovaries due to its proximity. Alternatively, a transabdominal ultrasound involves placing the probe on the lower abdomen, which may be less invasive but often yields less detailed images. The choice of method depends on patient comfort and the specific clinical context. It’s essential for technicians to measure follicle size and count accurately, as these parameters are critical for diagnosis. Patients should be informed that the procedure is generally painless and takes only about 15-30 minutes.
While ultrasound is a cornerstone in PCOS diagnosis, it is not without limitations. The Rotterdam criteria, widely used for PCOS diagnosis, require at least two out of three features: polycystic ovaries on ultrasound, hyperandrogenism (elevated male hormones), and irregular menstrual cycles. However, relying solely on ultrasound can lead to misdiagnosis, especially in lean women or those with milder symptoms, where ovarian appearance may not meet the strict criteria. Additionally, the interpretation of ultrasound images can vary among radiologists, emphasizing the need for experienced technicians. Despite these challenges, ultrasound remains a non-invasive, cost-effective, and widely available tool that, when combined with clinical and hormonal assessments, significantly enhances diagnostic accuracy.
A practical tip for patients undergoing ultrasound for PCOS evaluation is to ensure proper hydration before the procedure, as a full bladder can improve visualization in transabdominal scans. For those anxious about the process, understanding that the procedure is quick and carries no radiation risks can alleviate concerns. Clinicians should also consider the patient’s age and menstrual history, as ovarian morphology can vary with age, and adolescents may exhibit polycystic-like ovaries without meeting full PCOS criteria. In such cases, follow-up ultrasounds may be necessary to monitor changes over time. Ultimately, ultrasound serves as a critical first step in PCOS diagnosis, offering valuable insights into ovarian structure that guide subsequent treatment decisions.
Port Length Impact: Enhancing Sound Quality in Speaker Systems
You may want to see also
Frequently asked questions
Not always. While ultrasound is the primary tool for diagnosing polycystic ovary syndrome (PCOS), the appearance of polycystic ovaries can vary, and some cases may not be clearly visible depending on the severity or the individual's anatomy.
On an ultrasound, a polycystic ovary typically appears enlarged and contains 12 or more small follicles (fluid-filled sacs) measuring 2-9 mm in diameter, often arranged peripherally in a "string of pearls" pattern.
No, an ultrasound alone cannot definitively diagnose PCOS. Diagnosis requires a combination of criteria, including ultrasound findings, hormonal imbalances, and symptoms like irregular periods or excess androgen levels.
Polycystic ovaries may not appear on an ultrasound if the follicles are too small, the ovary is not enlarged, or the imaging technique is not sensitive enough. Additionally, early stages of PCOS or mild cases may not be detectable.