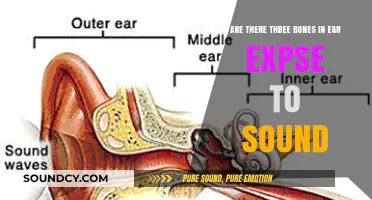
Constipation, a common gastrointestinal issue characterized by infrequent bowel movements or difficulty passing stools, often raises questions about associated symptoms, including bowel sounds. Bowel sounds, also known as borborygmi, are the noises produced by the movement of gas and fluids through the intestines. In constipated patients, the presence or absence of bowel sounds can provide valuable insights into the underlying mechanisms of the condition. While some individuals with constipation may exhibit hyperactive bowel sounds due to increased gas or fluid movement, others might have hypoactive or absent sounds, indicating reduced intestinal motility. Understanding these variations is crucial for healthcare providers to assess the severity of constipation and tailor appropriate treatment strategies.
Explore related products






What You'll Learn
![]()
Impact of Constipation on Bowel Sounds
Constipation often alters bowel sounds, but the nature of these changes can vary widely depending on the underlying cause and severity of the condition. Typically, bowel sounds in constipated patients may become hypoactive or even absent due to decreased intestinal motility. This occurs when the digestive system slows down, leading to reduced peristaltic movements. However, in some cases, hyperactive bowel sounds, known as borborygmi, can be present as the intestines struggle to move hardened stool. Understanding these variations is crucial for healthcare providers to accurately assess a patient’s condition and determine appropriate interventions.
To evaluate bowel sounds in constipated patients, auscultate the abdomen for at least 1–2 minutes, focusing on all four quadrants. Hypoactive sounds, characterized by fewer than 4–5 per minute, suggest slowed motility, while hyperactive sounds, exceeding 10 per minute, indicate increased effort by the intestines. For instance, a patient with opioid-induced constipation may exhibit hypoactive sounds due to the drug’s paralytic effect on the bowel. Conversely, a patient with constipation from irritable bowel syndrome might display hyperactive sounds as the intestines attempt to overcome obstruction. Pairing auscultation with a physical exam and patient history can provide a clearer diagnostic picture.
Practical tips for managing constipation-related bowel sound changes include increasing fiber intake (25–30 grams daily), staying hydrated (8–10 glasses of water per day), and incorporating physical activity. For acute cases, over-the-counter osmotic laxatives like polyethylene glycol (17g daily) or stimulant laxatives such as bisacodyl (5–15 mg) can be used, but long-term reliance should be avoided. Elderly patients or those on medications affecting motility (e.g., anticholinergics) require cautious monitoring, as their bowel sounds may not normalize quickly. Always reassess bowel sounds post-intervention to gauge effectiveness.
Comparatively, constipation-induced bowel sound changes differ from those in conditions like ileus or bowel obstruction. In ileus, bowel sounds are often absent due to complete cessation of motility, whereas partial obstruction may produce high-pitched, tinkling sounds. Constipation, however, typically presents with more subtle changes—either hypoactive or hyperactive sounds—depending on the stage and cause. Recognizing these distinctions ensures accurate diagnosis and prevents misinterpreting constipation as a more severe gastrointestinal issue.
In conclusion, constipation’s impact on bowel sounds is multifaceted, ranging from hypoactive to hyperactive patterns based on the underlying mechanism. Healthcare providers must correlate auscultation findings with clinical context, such as medication use, dietary habits, and patient history, to tailor treatment effectively. By addressing the root cause and monitoring bowel sounds during management, practitioners can improve patient outcomes and restore normal gastrointestinal function.
Unraveling the Mystery: What's Behind That Universal 'Oof' Sound?
You may want to see also
Explore related products






![]()
Normal vs. Abnormal Bowel Sound Patterns
Bowel sounds, often described as gurgling or rumbling noises, are a vital indicator of gastrointestinal activity. In a healthy individual, these sounds typically occur at a rate of 5 to 30 per minute, reflecting the normal movement of gas and fluids through the intestines. However, in constipated patients, the pattern and presence of bowel sounds can vary significantly, providing crucial insights into the underlying condition. Understanding the distinction between normal and abnormal bowel sound patterns is essential for accurate diagnosis and management.
Analyzing Normal Bowel Sounds:
Normal bowel sounds, known as borborygmi, are a sign of active peristalsis—the wave-like contractions that move food through the digestive tract. These sounds are typically soft, rhythmic, and evenly distributed across the abdomen. In a non-constipated individual, they indicate efficient digestion and elimination. For example, after a meal, bowel sounds may temporarily increase as the stomach and intestines work to process food. This pattern is reassuring and aligns with the body’s natural digestive processes.
Abnormal Patterns in Constipation:
In constipated patients, bowel sounds may become hypoactive (decreased) or hyperactive (increased), depending on the severity and cause of the condition. Hypoactive sounds, often described as faint or infrequent, suggest slowed intestinal motility, a common feature of constipation. Conversely, hyperactive sounds, which are louder and more frequent, may indicate irritable bowel syndrome (IBS) with constipation or an obstructive process. For instance, a patient with fecal impaction might exhibit hyperactive sounds as the intestines attempt to overcome the blockage.
Practical Tips for Assessment:
To accurately assess bowel sounds in constipated patients, use a stethoscope and listen to all four quadrants of the abdomen for at least 1–2 minutes. Note the frequency, pitch, and location of the sounds. If sounds are absent or minimal, consider re-evaluating after the patient has attempted to pass stool or after administering a mild laxative (e.g., 17g of polyethylene glycol 3350 in 8 oz of water). Document any changes, as they can guide treatment decisions, such as increasing fiber intake (25–30g daily) or prescribing prokinetic agents.
Clinical Takeaway:
While bowel sounds are present in constipated patients, their pattern often deviates from the norm. Hypoactive sounds are more common and align with the sluggish motility seen in constipation, whereas hyperactive sounds may signal complications. Clinicians should interpret these findings in conjunction with symptoms, medical history, and physical exam results. For example, a patient with hypoactive sounds and abdominal distension may benefit from a stool softener, while hyperactive sounds with cramping could warrant further investigation for IBS or obstruction. Recognizing these patterns enhances diagnostic accuracy and tailors treatment to the patient’s specific needs.
Unveiling the Unique and Hilarious Call of Kookaburras in Nature
You may want to see also
Explore related products





![]()
How Constipation Alters Intestinal Motility
Constipation fundamentally disrupts the rhythmic contractions of the intestines, known as peristalsis, which propel food and waste through the digestive tract. Normally, these wave-like movements occur at a steady pace, ensuring efficient transit. However, in constipation, this motility slows significantly, often due to weakened or uncoordinated muscle contractions. This delay allows stool to harden as excess water is absorbed, making it difficult to pass. The result is a vicious cycle: harder stool requires stronger contractions, which the compromised motility cannot provide, further exacerbating the issue.
To understand the impact, consider the role of the enteric nervous system (ENS), often called the "second brain," which regulates intestinal motility. In constipation, the ENS may become dysregulated, leading to abnormal nerve signaling. This can manifest as either reduced frequency of contractions or prolonged intervals between them. For instance, studies show that patients with chronic constipation often exhibit slower colonic transit times, sometimes taking 72 hours or more for stool to move through the colon compared to the typical 24–48 hours. This delay is a direct consequence of impaired motility.
Practical interventions to restore motility include dietary and lifestyle modifications. Increasing fiber intake (25–30 grams daily) and staying hydrated (2–3 liters of water) can soften stool and stimulate contractions. Physical activity, such as 30 minutes of daily walking, enhances abdominal muscle tone and promotes peristalsis. For severe cases, prokinetic medications like prucalopride (1–2 mg daily) may be prescribed to directly stimulate intestinal contractions. However, these should be used under medical supervision, as overuse can lead to dependency or electrolyte imbalances.
Comparatively, constipation differs from conditions like irritable bowel syndrome (IBS) with constipation (IBS-C), where motility issues are often accompanied by visceral hypersensitivity. In IBS-C, the ENS may overreact, causing spasms rather than slow transit. This distinction highlights why a one-size-fits-all approach fails. For example, while fiber helps constipation, it can worsen symptoms in IBS-C due to increased gas production. Tailored strategies, such as soluble fiber (psyllium) for constipation versus insoluble fiber (wheat bran) for mild cases, are crucial for effective management.
Finally, monitoring bowel sounds provides a non-invasive way to assess motility. In constipation, bowel sounds may be hypoactive or absent due to reduced intestinal activity. However, paradoxically, high-pitched or hyperactive sounds can occur if the body attempts to compensate for slow transit. Clinicians often use this auditory cue alongside patient history and imaging (e.g., abdominal X-rays) to diagnose motility disorders. For home management, tracking bowel habits and correlating them with dietary changes can offer insights into motility patterns, guiding personalized interventions.
Do You Need a Sound Card for Your Gaming PC?
You may want to see also
Explore related products






![]()
Clinical Significance of Present Bowel Sounds
Bowel sounds, often described as gurgling or rumbling noises, are produced by the movement of gas and fluid through the intestines. In a constipated patient, the presence or absence of these sounds can provide critical insights into the underlying pathophysiology. Contrary to common misconceptions, bowel sounds are not always diminished in constipation. In fact, hyperactive or high-pitched sounds may indicate an ileus or early obstruction, while normal or increased sounds can reflect ongoing peristalsis despite delayed transit. This variability underscores the importance of interpreting bowel sounds within the broader clinical context.
Clinically, present bowel sounds in a constipated patient can rule out mechanical obstruction, a life-threatening condition requiring immediate intervention. For instance, a patient with constipation and absent bowel sounds may warrant urgent imaging, such as an abdominal X-ray or CT scan, to evaluate for obstruction. Conversely, the presence of sounds suggests functional constipation or opioid-induced constipation, where motility is preserved but transit is slowed. This distinction is crucial for guiding management, as functional constipation typically responds to dietary modifications, hydration, and laxatives, whereas obstruction necessitates surgical or endoscopic intervention.
The auscultation technique itself is pivotal in accurately assessing bowel sounds. Clinicians should listen in all four quadrants for at least 1–2 minutes, as sounds may be intermittent. A stethoscope with a diaphragm is preferred for detecting higher-pitched sounds, while the bell can capture lower frequencies. In constipated patients, documenting the character (e.g., hyperactive, hypoactive) and frequency of sounds provides a baseline for monitoring progression or resolution. For example, a shift from hyperactive to hypoactive sounds may signal evolving obstruction, prompting reevaluation.
Pediatric and elderly populations require special consideration when interpreting bowel sounds in constipation. In infants, absent or diminished sounds may indicate Hirschsprung’s disease or meconium ileus, while hyperactive sounds could suggest necrotizing enterocolitis. In the elderly, medication-induced constipation (e.g., from calcium channel blockers or anticholinergics) often coexists with normal bowel sounds. Clinicians should correlate findings with risk factors, such as medication history or prior abdominal surgery, to tailor management. For instance, polyethylene glycol (17–35 g/day) is a first-line laxative in opioid-induced constipation, while methylnaltrexone (0.15 mg/kg subcutaneously) may be used in refractory cases.
In summary, present bowel sounds in a constipated patient are not merely reassuring but diagnostically significant. They differentiate functional constipation from obstruction, guide treatment selection, and inform monitoring strategies. By integrating auscultation findings with clinical history and risk factors, healthcare providers can optimize care, avoiding both over- and under-treatment. This nuanced approach ensures timely intervention while minimizing unnecessary procedures, highlighting the clinical significance of bowel sounds in constipation management.
Understanding the Causes and Fixes for Code P0725 Engine Noise
You may want to see also
Explore related products






![]()
Diagnostic Approach in Constipated Patients
Bowel sounds, often described as gurgling or rumbling noises, are a key indicator of gastrointestinal activity. In constipated patients, these sounds can vary widely, from hyperactive to hypoactive, depending on the underlying cause. Understanding this variability is crucial for a targeted diagnostic approach.
Step 1: Assess Bowel Sound Patterns
Begin by auscultating the abdomen in all four quadrants for 1–2 minutes. Hyperactive bowel sounds (loud, frequent) may suggest ileus or early obstruction, while hypoactive or absent sounds could indicate adynamic ileus or advanced obstruction. Normal or slightly decreased sounds are common in functional constipation. Document the pattern and correlate it with the patient’s symptoms, such as abdominal pain, bloating, or vomiting, to narrow the differential diagnosis.
Step 2: Evaluate Clinical Context
Consider patient-specific factors: age, medication use, dietary habits, and comorbidities. For instance, older adults on opioids or anticholinergics are at higher risk for medication-induced constipation. In children, constipation often stems from dietary fiber deficiency or behavioral issues. A thorough history, including stool frequency, consistency (Bristol Stool Chart Types 1–2), and straining, helps differentiate between functional and organic causes.
Step 3: Perform Focused Physical Examination
Inspect for abdominal distension, palpable masses, or tenderness. Digital rectal examination (DRE) is essential to assess stool burden, rectal tone, and occult blood. A rectal vault filled with hard stool confirms constipation, while a empty vault with normal tone suggests obstructed defecation. Be cautious in patients with suspected bowel obstruction, as DRE may precipitate perforation.
Step 4: Order Targeted Investigations
Start with simple tests: abdominal X-ray to identify fecal loading or obstruction, and thyroid function tests to rule out hypothyroidism. In chronic cases, consider colonoscopy to exclude structural abnormalities like colorectal cancer or strictures. For suspected dyssynergic defecation, anorectal manometry or defecography provides definitive evidence. Avoid over-investigation in uncomplicated cases, as this increases costs and patient anxiety.
Cautions and Practical Tips
Avoid misinterpreting bowel sounds in isolation; they are nonspecific and must be contextualized. For example, absent sounds in a patient with acute abdominal pain warrant urgent imaging to rule out strangulated obstruction. Encourage patients to maintain a symptom diary, noting stool patterns, dietary changes, and medication use, to aid diagnosis. Hydration and fiber supplementation (25–30 g/day) are first-line interventions, but monitor for worsening symptoms, which may indicate underlying pathology.
By systematically integrating bowel sound assessment with clinical and diagnostic data, clinicians can effectively differentiate between benign and serious causes of constipation, ensuring appropriate management and improved patient outcomes.
Understanding Sound Patterns: The Building Blocks of Language and Music
You may want to see also
Frequently asked questions
Bowel sounds may vary in a constipated patient. While some individuals may have normal or increased bowel sounds due to increased intestinal activity, others may have decreased or absent sounds due to slowed motility.
Present bowel sounds in a constipated patient can indicate ongoing intestinal activity, but they do not necessarily rule out constipation. The presence of sounds suggests the intestines are still functioning, though possibly inefficiently.
Absent bowel sounds can be a concern in constipation, as they may indicate ileus (paralysis of the intestines) or severe obstruction. However, absent sounds alone are not diagnostic and require further evaluation.
In constipation, bowel sounds may be hyperactive (high-pitched and frequent) due to increased effort to move stool, or hypoactive (decreased or absent) due to slowed motility. Normal bowel sounds are typically moderate and consistent.