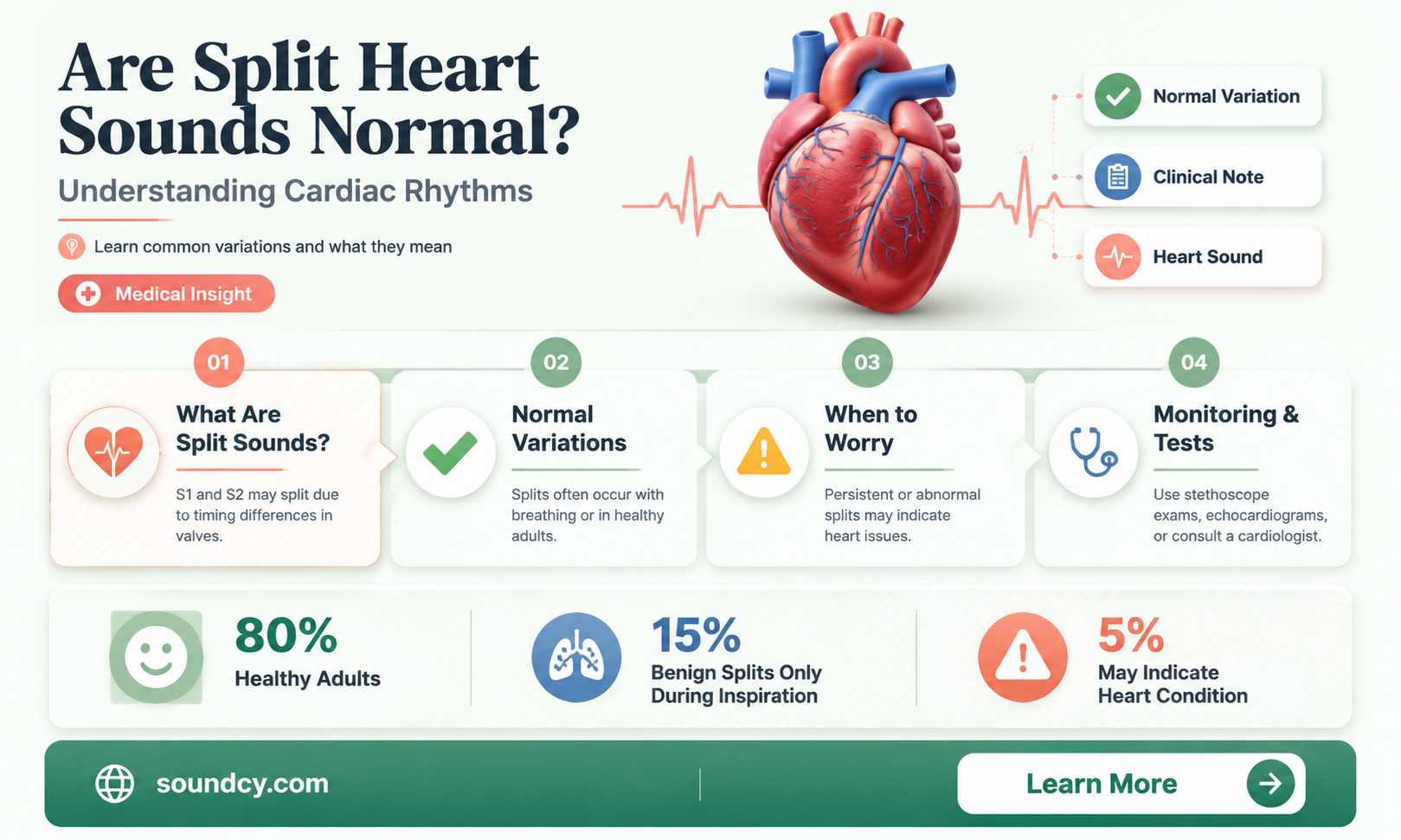
Split heart sounds, also known as physiological splitting, refer to the normal variation in the timing of heart valve closures during the cardiac cycle. This phenomenon is most commonly observed in the second heart sound (S2), which consists of the closure of the aortic and pulmonic valves. Under certain conditions, such as during inspiration, the pulmonic valve closes slightly later than the aortic valve, resulting in a split S2. This is considered a normal physiological process and is more pronounced in children and young adults. However, persistent or abnormal splitting may indicate underlying cardiac issues, such as valvular dysfunction or pulmonary hypertension, necessitating further evaluation by a healthcare professional.
| Characteristics | Values |
|---|---|
| Definition | Split heart sounds refer to the separation of the first (S1) and second (S2) heart sounds, often heard as a "splitting" of S2. |
| Normalcy | Split S2 is normal in certain conditions, particularly during inspiration in healthy individuals. |
| Physiological Basis | During inspiration, the decreased intrathoracic pressure delays the closure of the pulmonary valve, causing the aortic component of S2 to close first, followed by the pulmonary component. |
| Types of Splitting | Physiological splitting: Normal, wide splitting during inspiration. Pathological splitting: Persistent or wide splitting during expiration, indicating potential underlying issues. |
| Associated Conditions | Normal in healthy individuals, especially young adults. Pathological splitting may be linked to conditions like right bundle branch block, pulmonary hypertension, or atrial septal defect. |
| Clinical Significance | Physiological splitting is benign. Pathological splitting requires further evaluation to identify underlying cardiac or pulmonary disorders. |
| Diagnostic Approach | Auscultation during both inspiration and expiration. Further tests (e.g., ECG, echocardiogram) may be needed for pathological cases. |
| Treatment | No treatment needed for physiological splitting. Treatment of underlying condition for pathological splitting. |
Explore related products






What You'll Learn
![]()
Understanding Split Heart Sounds
Split heart sounds, also known as split S2, occur when the second heart sound (S2) is divided into two distinct components rather than being heard as a single sound. This phenomenon is primarily related to the closure of the aortic and pulmonary valves, which normally occur almost simultaneously. However, under certain conditions, the closure times of these valves can become slightly separated, leading to a split S2. While this can be a normal finding in specific circumstances, it is essential to understand when it is benign and when it may indicate an underlying issue.
In healthy individuals, a physiological split S2 can be heard during inspiration, particularly in children and young adults. This occurs because during inspiration, intrathoracic pressure decreases, causing the right ventricle to eject blood more slowly and delaying the closure of the pulmonary valve. As a result, the pulmonary component (P2) of S2 is heard slightly after the aortic component (A2), creating a split sound. This type of split is considered normal and typically disappears upon expiration. Recognizing this physiological split is crucial for distinguishing it from pathological causes.
Pathological split heart sounds, on the other hand, may indicate conditions such as right bundle branch block, pulmonary hypertension, or atrial septal defects. In these cases, the split S2 is often wide and persistent, meaning it does not resolve during expiration. For example, in right bundle branch block, delayed electrical activation of the right ventricle leads to delayed contraction and closure of the pulmonary valve, causing a consistently split S2. Understanding the context and characteristics of the split—whether it is inspiratory, expiratory, or persistent—is key to determining its significance.
Clinicians assess split heart sounds by carefully auscultating the precordium, noting the timing and duration of the split during the respiratory cycle. Patients may be asked to breathe deeply to observe changes in the split S2. Additionally, other clinical findings, such as murmurs or changes in heart rhythm, can provide further clues to the underlying cause. While a physiological split S2 is harmless, a pathological split warrants further investigation, including electrocardiograms, echocardiograms, or other diagnostic tests to identify the root cause.
In summary, split heart sounds are not inherently abnormal but require careful evaluation to determine their significance. A physiological split S2 during inspiration is a normal variant, particularly in younger individuals, while a persistent or wide split may signal an underlying cardiac condition. Healthcare providers must remain vigilant in their auscultation and consider the patient’s medical history and other clinical findings to differentiate between benign and pathological splits. By understanding the nuances of split heart sounds, clinicians can ensure accurate diagnosis and appropriate management.
Exploring the Unique and Varied Sounds of Frogs in Nature
You may want to see also
Explore related products


$31.99 $34.99




![]()
Causes of Split Heart Sounds
Split heart sounds, also known as split S2, occur when the second heart sound (S2) is divided into two distinct components, creating an abnormal splitting effect. This phenomenon is not always a cause for concern, but understanding its underlying causes is essential for proper diagnosis and management. One of the primary causes of split heart sounds is respiration-induced changes, which are often considered normal. During inspiration, the chest cavity expands, leading to decreased intrathoracic pressure and delayed closure of the pulmonary valve. This results in a widened split between the aortic (A2) and pulmonary (P2) components of S2, known as a physiological split. Conversely, during expiration, the split narrows or disappears. This type of splitting is benign and commonly observed in children and young adults.
Another cause of split heart sounds is right bundle branch block (RBBB), a cardiac conduction abnormality. In RBBB, the electrical impulse is delayed in the right ventricle, causing it to contract later than the left ventricle. This delay leads to a widened or fixed splitting of S2, as the pulmonary valve closes later than the aortic valve. Unlike the physiological split, this type of splitting does not vary with respiration and is often accompanied by other signs of RBBB on an electrocardiogram (ECG). While RBBB can be congenital or age-related, it may also indicate underlying heart disease, such as cardiomyopathy or ischemia, requiring further evaluation.
Atrial septal defect (ASD) is another significant cause of split heart sounds. In ASD, a hole in the atrial septum allows oxygenated blood to flow from the left atrium to the right atrium. This increases blood volume in the right ventricle, leading to delayed closure of the pulmonary valve and a widened or fixed splitting of S2. Patients with ASD may also exhibit other signs, such as a systolic murmur or right ventricular heave. Early diagnosis and intervention are crucial to prevent complications like pulmonary hypertension.
Pulmonary hypertension itself can also cause split heart sounds. Elevated pressure in the pulmonary artery delays the closure of the pulmonary valve, resulting in a widened splitting of S2. This type of splitting is often accompanied by a loud P2 component and may indicate severe underlying conditions, such as chronic lung disease or congenital heart defects. Prompt evaluation and management are essential to address the root cause and prevent further deterioration of cardiac function.
Lastly, left bundle branch block (LBBB) can occasionally cause split heart sounds, although it is less common than RBBB. In LBBB, the delayed contraction of the left ventricle can affect the timing of aortic valve closure, potentially leading to abnormal splitting of S2. However, this is usually overshadowed by other characteristic findings of LBBB, such as a widened QRS complex on ECG. Understanding these causes is critical for differentiating between normal and pathological split heart sounds, ensuring appropriate patient care.
Exploring the Iconic, Nostalgic Sounds of Pac-Man's Classic Gameplay
You may want to see also
Explore related products






![]()
Normal vs. Abnormal Splitting
Normal Splitting of Heart Sounds
In a healthy individual, the splitting of the second heart sound (S2) is a common and benign phenomenon, particularly during inspiration. S2 is composed of two components: the closure of the pulmonary valve (P2) and the aortic valve (A2). During inspiration, the intrathoracic pressure decreases, causing the right ventricle to fill with more blood and delay the closure of the pulmonary valve. This results in a widened split between A2 and P2, known as physiological splitting. This splitting is normal and disappears during expiration when intrathoracic pressure increases, causing P2 and A2 to coincide more closely. Physiological splitting is typically heard loudest in the second left intercostal space (aortic area) and the third left intercostal space (pulmonic area). It is a sign of a healthy cardiovascular system and does not indicate pathology.
Abnormal Splitting: Fixed Splitting
Abnormal splitting occurs when the S2 components remain split throughout both inspiration and expiration, a condition known as fixed splitting. This is often observed in conditions that cause a delay in the closure of the right-sided heart valves, such as right bundle branch block (RBBB) or pulmonary hypertension. In RBBB, the delayed electrical activation of the right ventricle leads to delayed contraction and closure of the pulmonary valve, causing P2 to lag behind A2 consistently. Similarly, in pulmonary hypertension, increased pressure in the pulmonary artery delays pulmonary valve closure, resulting in fixed splitting. Fixed splitting is abnormal and warrants further investigation to identify the underlying cause.
Abnormal Splitting: Reversed Splitting
Another abnormal pattern is reversed splitting, where the S2 components are closer together during inspiration and wider during expiration. This occurs in conditions that delay the closure of the aortic valve, such as left bundle branch block (LBBB) or aortic stenosis. In LBBB, the delayed activation of the left ventricle causes the aortic valve to close later, making A2 lag behind P2 during expiration. Aortic stenosis, where the aortic valve is narrowed, also delays aortic valve closure, leading to reversed splitting. Reversed splitting is a red flag and requires prompt evaluation to address the underlying cardiac issue.
Clinical Implications and Diagnosis
Distinguishing between normal and abnormal splitting is crucial for accurate diagnosis. Normal splitting is a physiological variation, while abnormal splitting (fixed or reversed) indicates significant cardiac pathology. Auscultation remains the primary tool for detecting splitting, with careful attention to the timing and duration of S2 components during both phases of respiration. Additional diagnostic tests, such as electrocardiography (ECG) or echocardiography, may be necessary to confirm the underlying cause of abnormal splitting. Clinicians should remain vigilant, as abnormal splitting can be an early indicator of conditions like bundle branch blocks, valvular disease, or pulmonary hypertension.
Key Takeaways
Normal splitting of S2 is a physiological phenomenon observed during inspiration, reflecting healthy cardiovascular function. In contrast, abnormal splitting (fixed or reversed) is a pathological sign that requires further investigation. Understanding the differences between normal and abnormal splitting is essential for accurate diagnosis and timely intervention. Clinicians should correlate auscultation findings with patient history and additional diagnostic tools to ensure comprehensive care.
Audiophiles vs Casual Listeners: Who Needs Sound Quality?
You may want to see also
Explore related products





![]()
Diagnosis and Evaluation Methods
When evaluating whether split heart sounds are normal, healthcare providers employ a variety of diagnostic and evaluation methods to assess the underlying cause and clinical significance. The first step typically involves a thorough physical examination, during which the clinician uses a stethoscope to listen to heart sounds (auscultation). Split heart sounds, particularly a split second heart sound (S2), are assessed for their duration, intensity, and variability with respiration. A normal S2 split is physiological and often widens during inspiration, especially in healthy individuals, due to changes in intrathoracic pressure affecting the pulmonary and aortic valve closure times. However, a persistent or abnormal split, such as a paradoxical split (widening during expiration), may indicate underlying conditions like left bundle branch block or pulmonary hypertension.
Electrocardiography (ECG) is another essential tool in the evaluation process. It helps identify conduction abnormalities, such as right or left bundle branch block, which can cause abnormal splitting of heart sounds. ECG findings, combined with auscultation, provide a more comprehensive understanding of the heart's electrical and mechanical function. For instance, a widened QRS complex on ECG, coupled with a paradoxical S2 split, strongly suggests a conduction disorder that requires further investigation.
Echocardiography is a cornerstone in diagnosing the cause of split heart sounds. This non-invasive imaging technique provides detailed visualization of the heart's structure and function, including valve morphology, chamber sizes, and blood flow patterns. It can identify conditions like pulmonary hypertension, valvular disease, or congenital heart defects that may contribute to abnormal splitting. Doppler echocardiography is particularly useful for assessing pressure gradients and valve function, which are critical in determining the severity and etiology of the split sounds.
In cases where the cause remains unclear, chest X-rays or cardiac MRI may be employed to evaluate the thoracic anatomy and rule out structural abnormalities. A chest X-ray can reveal signs of pulmonary congestion, enlarged chambers, or other abnormalities that might explain the split heart sounds. Cardiac MRI offers high-resolution images of the heart's structure and can detect subtle changes in tissue characteristics, such as fibrosis or inflammation, which may not be apparent on echocardiography.
Finally, invasive diagnostic procedures like cardiac catheterization may be necessary in complex cases, particularly when pulmonary hypertension or coronary artery disease is suspected. This procedure allows for direct measurement of pressures within the heart chambers and vessels, providing definitive data to guide treatment. However, it is reserved for patients with high clinical suspicion of severe underlying pathology, as it carries greater risks compared to non-invasive methods.
In summary, the diagnosis and evaluation of split heart sounds involve a systematic approach, starting with physical examination and progressing to advanced imaging and invasive testing as needed. Each method plays a critical role in differentiating between normal physiological splitting and pathological conditions, ensuring appropriate management and patient care.
Understanding Sound FX Volume: Balancing Audio Effects in Media Production
You may want to see also
Explore related products






![]()
Clinical Significance and Treatment
Split heart sounds, particularly split S2, are a common finding in clinical practice and can be normal under certain physiological conditions. However, their presence or absence can also provide critical insights into a patient’s cardiovascular health, making their clinical significance and appropriate treatment essential to understand. Split heart sounds occur when the aortic and pulmonary components of the second heart sound (S2) are widely separated, often heard as distinct "dups" rather than a single sound. This phenomenon is influenced by factors such as respiratory phase, age, and underlying cardiac conditions.
Clinical Significance: In many cases, a physiological split S2 is benign and reflects normal variations in heart function. It is commonly heard in children and young adults, where the timing of aortic and pulmonary valve closure differs slightly. During inspiration, the split widens as the intrathoracic pressure decreases, delaying pulmonary valve closure. Conversely, during expiration, the split narrows or disappears. However, a persistently split S2 or one that does not vary with respiration may indicate pathological conditions. For instance, a wide and fixed split S2 is a hallmark of right bundle branch block (RBBB) or atrial septal defect (ASD), where delayed right ventricular emptying alters the timing of pulmonary valve closure. Additionally, a paradoxical split S2 (widening during expiration) suggests conditions like pulmonary hypertension or left bundle branch block (LBBB).
Diagnostic Approach: When encountering split heart sounds, clinicians should first determine whether the split is physiological or pathological. A detailed history, physical examination, and auscultation during both inspiration and expiration are crucial. If the split is abnormal or fixed, further diagnostic tests such as electrocardiography (ECG), chest X-ray, and echocardiography may be warranted to identify underlying cardiac abnormalities. In cases of suspected pulmonary hypertension or congenital heart disease, additional imaging or hemodynamic studies may be necessary.
Treatment Considerations: The treatment of split heart sounds is directed at addressing the underlying cause rather than the sound itself. For physiological splits, no intervention is required. In pathological cases, management depends on the etiology. For example, patients with RBBB or LBBB may require monitoring for associated cardiovascular risks, while those with ASD or pulmonary hypertension may need surgical repair or targeted pharmacotherapy. In pulmonary hypertension, medications like vasodilators or prostacyclin analogs may be prescribed to improve symptoms and slow disease progression.
Patient Education and Monitoring: Educating patients about the nature of split heart sounds and their clinical implications is vital. Patients with benign splits should be reassured, while those with pathological splits need to understand the importance of follow-up care and adherence to treatment plans. Regular monitoring, including repeat auscultation and diagnostic testing, is essential to assess disease progression or response to therapy. Early detection and management of underlying conditions can prevent complications and improve long-term outcomes.
In summary, while split heart sounds can be normal, their clinical significance lies in their ability to reveal underlying cardiac pathology. A systematic approach to diagnosis and treatment, tailored to the specific etiology, ensures optimal patient care. Clinicians must remain vigilant in evaluating these sounds, as they can serve as an early indicator of potentially serious cardiovascular conditions.
How Stethoscopes Amplify Sound: Unveiling the Science Behind Acoustic Enhancement
You may want to see also
Frequently asked questions
No, split heart sounds are not always abnormal. Physiological splitting of the second heart sound (S2) can occur during inspiration and is considered normal. However, pathological splitting may indicate underlying heart conditions.
Normal splitting of S2 occurs due to differences in the timing of aortic and pulmonary valve closure during inspiration, which delays pulmonary valve closure and creates a temporary split sound.
Split heart sounds are concerning if they are wide, fixed (present during both inspiration and expiration), or accompanied by other symptoms like shortness of breath, chest pain, or murmurs, as these may indicate heart valve disorders or congenital conditions.