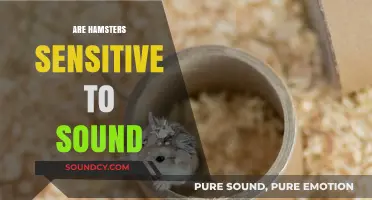
Heart sounds are a critical component of the physical examination and are frequently tested on the United States Medical Licensing Examination (USMLE). Understanding the characteristics of normal and abnormal heart sounds, including S1, S2, murmurs, and extra heart sounds, is essential for medical students preparing for the exam. The USMLE often assesses the ability to differentiate between various cardiac conditions based on auscultation findings, making it crucial for test-takers to master this skill. Familiarity with the physiology, pathophysiology, and clinical significance of heart sounds ensures not only exam success but also competence in real-world patient care.
| Characteristics | Values |
|---|---|
| Presence on USMLE | Yes, heart sounds are tested on both USMLE Step 1 and Step 2 CK. |
| Key Heart Sounds | S1 (first heart sound), S2 (second heart sound), S3, S4, murmurs. |
| S1 Characteristics | Low-pitched, longer duration, associated with mitral and tricuspid closure. |
| S2 Characteristics | High-pitched, shorter duration, associated with aortic and pulmonic closure. |
| S3 Characteristics | Low-pitched, occurs in early diastole, often benign in children, pathological in adults. |
| S4 Characteristics | Low-pitched, occurs in late diastole, indicates stiff ventricle (e.g., hypertension, left ventricular hypertrophy). |
| Murmurs | Classified by timing (systolic/diastolic), intensity (Grade 1-6), location, and quality. |
| Clinical Relevance | Assessed for valvular disease, congenital heart defects, and cardiac function. |
| Exam Focus | Identification, characteristics, and clinical correlations of heart sounds. |
| Study Resources | Online auscultation tools, USMLE review books, and practice questions. |
| Weightage | Moderate importance in cardiology-related questions on USMLE exams. |
Explore related products






What You'll Learn
- Normal Heart Sounds: Understanding S1, S2, and their characteristics in a healthy heart
- Murmurs Classification: Differentiating innocent, pathologic murmurs, and their clinical significance
- Extra Heart Sounds: Identifying S3, S4 gallops and their implications
- Valvular Lesions: Correlating heart sounds with specific valve diseases
- Exam Techniques: Proper auscultation methods and common USMLE case scenarios
![]()
Normal Heart Sounds: Understanding S1, S2, and their characteristics in a healthy heart
Normal heart sounds are a fundamental aspect of cardiovascular assessment and are indeed a crucial topic on the USMLE. Understanding the characteristics of these sounds, particularly S1 and S2, is essential for any medical professional. The heart typically produces two main sounds, often described as "lub-dub," which correspond to the closure of the heart valves during the cardiac cycle. These sounds provide valuable insights into the heart's function and can indicate the presence of various cardiac conditions when abnormal.
S1 (First Heart Sound): This sound is the first component of the familiar "lub-dub" and is primarily associated with the closure of the atrioventricular (AV) valves, namely the mitral and tricuspid valves. S1 occurs at the beginning of systole, marking the onset of ventricular contraction. It is typically low in pitch and longer in duration compared to S2. The mitral component of S1 is usually louder and occurs slightly before the tricuspid component due to the higher pressure in the left heart. In a healthy heart, S1 is best heard at the apex of the heart, which is located in the fifth left intercostal space, mid-clavicular line.
S2 (Second Heart Sound): The second heart sound, or S2, is the "dub" in the cardiac cycle and signifies the closure of the semilunar valves—the aortic and pulmonary valves. This sound marks the end of ventricular systole and the beginning of diastole. S2 is higher in pitch and shorter in duration than S1. It is composed of two components: the aortic and pulmonary valve closures. The aortic component (A2) is usually louder and occurs slightly after the pulmonary component (P2) due to the higher pressure in the aorta. S2 is best auscultated at the base of the heart, particularly at the second right intercostal space for the aortic valve and the second left intercostal space for the pulmonary valve.
In a normal heart, the intensity and timing of S1 and S2 are consistent and follow a predictable pattern. S1 is typically louder than S2, and the split between the two components of S2 (A2 and P2) is usually narrow and may vary with respiration. During inspiration, the intrathoracic pressure decreases, leading to a slight delay in the closure of the pulmonary valve, causing a wider splitting of S2. This physiological splitting is more noticeable in children and young adults.
Understanding the characteristics of normal heart sounds is vital for identifying abnormalities. For instance, a loud and palpable S1 could suggest volume overload or mitral stenosis, while a widely split S2 that doesn't vary with respiration may indicate a right bundle branch block or pulmonary hypertension. Thus, a comprehensive knowledge of S1 and S2 is essential for medical students and professionals to interpret cardiac auscultation findings accurately, especially in the context of the USMLE.
Accessing Sound Select in SM64: A Step-by-Step Guide for Gamers
You may want to see also
Explore related products






![]()
Murmurs Classification: Differentiating innocent, pathologic murmurs, and their clinical significance
Heart murmurs are common findings during cardiac auscultation and are classified into innocent (benign) murmurs and pathologic murmurs. Differentiating between these types is crucial for appropriate clinical management. Innocent murmurs are functional, occur in structurally normal hearts, and do not require intervention. They are often soft (grade I-III/VI), short in duration, and may be associated with physiologic states such as pregnancy, anemia, or fever. For example, Still’s murmur in children is a classic innocent murmur, characterized by a vibratory, musical quality during mid-systole. Innocent murmurs typically do not produce symptoms, do not change over time, and are not associated with abnormal hemodynamics.
Pathologic murmurs, in contrast, result from structural heart abnormalities, such as valvular disease, septal defects, or hypertrophy. These murmurs are often louder (grade III/VI or greater), longer in duration, and may be associated with symptoms like chest pain, shortness of breath, or syncope. For instance, a systolic ejection murmur in a patient with aortic stenosis is pathologic, reflecting turbulent blood flow across a narrowed valve. Pathologic murmurs may also be accompanied by abnormal heart sounds, such as S3 or S4 gallops, or signs of heart failure. Their clinical significance lies in their ability to indicate underlying cardiac disease requiring further evaluation and treatment.
Classification of murmurs relies on timing (systolic vs. diastolic), location, radiation, intensity, pitch, and quality. Systolic murmurs are further categorized into ejection murmurs (e.g., aortic stenosis, hypertrophic cardiomyopathy) and regurgitant murmurs (e.g., mitral regurgitation). Diastolic murmurs are typically associated with valvular stenosis (e.g., aortic or mitral stenosis) or regurgitation (e.g., aortic regurgitation). For example, a high-pitched, crescendo-decrescendo murmur heard best at the right second intercostal space suggests aortic stenosis, while a low-pitched, rumbling diastolic murmur at the apex indicates mitral stenosis.
Clinical significance is determined by the murmur’s characteristics and the patient’s symptoms. Innocent murmurs are reassuring and do not warrant extensive workup, whereas pathologic murmurs require further evaluation with imaging (e.g., echocardiography) and potential intervention. For USMLE purposes, understanding the auscultatory findings, associated conditions, and management is essential. For instance, a harsh systolic murmur in a child with a hyperactive precordium may suggest ventricular septal defect, while a soft, flow-related murmur in an asymptomatic adolescent is likely innocent.
In summary, differentiating between innocent and pathologic murmurs hinges on auscultatory features, patient context, and associated symptoms. Innocent murmurs are benign and require no intervention, while pathologic murmurs signify underlying cardiac disease and necessitate further evaluation. Mastery of murmur classification and clinical significance is critical for USMLE success and clinical practice, ensuring accurate diagnosis and appropriate patient management.
Samsung Gear Sport SM-R600: Sound or Silence?
You may want to see also
Explore related products

![Cardiac/Vascular Nurse Exam Secrets Study Guide - Exam Review and Practice Test for the Cardiac/Vascular Nurse Test: [2nd Edition]](https://m.media-amazon.com/images/I/71u5HTFHFHL._AC_UY218_.jpg)

![CSC Exam Study Guide: Secrets Review Book and Practice Test Questions for the Cardiac Surgery Certification: [2nd Edition]](https://m.media-amazon.com/images/I/61W7dQxSaAL._AC_UY218_.jpg)


![]()
Extra Heart Sounds: Identifying S3, S4 gallops and their implications
Extra heart sounds, specifically S3 and S4 gallops, are important clinical findings that can provide valuable insights into a patient’s cardiac function. These sounds are not part of the normal lub-dub (S1 and S2) heart sounds but are additional auditory clues that signify underlying pathophysiology. Identifying and interpreting these sounds correctly is crucial, especially in the context of the USMLE, where understanding their implications can differentiate between diagnoses. Both S3 and S4 gallops are diastolic sounds, occurring after the aortic valve closes (S2), but their timing, characteristics, and associated conditions differ significantly.
The S3 gallop, often described as a "ventricular gallop," is a low-pitched sound heard in early diastole, approximately 0.12 to 0.18 seconds after S2. It is best auscultated with the patient in the left lateral decubitus position using the bell of the stethoscope over the apex of the heart. An S3 is typically associated with increased ventricular filling, which can occur in both pathological and physiological states. Pathologically, it is commonly heard in conditions such as heart failure with reduced ejection fraction (HFrEF), severe mitral or aortic regurgitation, and acute myocardial infarction. Physiologically, it may be present in children, young adults, or well-trained athletes due to increased stroke volume. On the USMLE, recognizing an S3 gallop should prompt consideration of volume overload or systolic dysfunction.
In contrast, the S4 gallop is a late diastolic sound, occurring just before S1, and is often described as an "atrial gallop." It is high-pitched and best heard with the diaphragm of the stethoscope at the cardiac apex, often more audible with the patient in the supine position. An S4 indicates stiff or noncompliant ventricles, leading to increased atrial effort to fill the ventricle. This sound is commonly associated with conditions such as hypertension, aortic stenosis, left ventricular hypertrophy, and coronary artery disease. On the USMLE, an S4 gallop should raise suspicion of diastolic dysfunction or increased ventricular stiffness, often seen in older patients with long-standing hypertension or ischemic heart disease.
Distinguishing between S3 and S4 gallops is essential for accurate diagnosis. A helpful mnemonic is that an S3 gallop is heard with the phrase "Kentucky" (S1, S2, S3), while an S4 gallop aligns with "Tennessee" (S4, S1, S2). Additionally, the context of the patient’s history and other clinical findings is critical. For example, an S3 in a young athlete is likely benign, whereas an S3 in an elderly patient with dyspnea and peripheral edema strongly suggests heart failure. Similarly, an S4 in a patient with uncontrolled hypertension is a red flag for left ventricular hypertrophy and increased cardiovascular risk.
In the context of the USMLE, extra heart sounds are high-yield topics that test both auscultation skills and clinical reasoning. Understanding the mechanisms behind S3 and S4 gallops, their characteristic sounds, and their associated conditions is vital. For instance, a vignette describing a patient with a low-pitched sound after S2 in early diastole should lead to the identification of an S3 gallop and consideration of heart failure. Conversely, a high-pitched sound just before S1 in a patient with hypertension points to an S4 gallop and diastolic dysfunction. Mastery of these concepts ensures not only exam success but also clinical competence in diagnosing and managing cardiac pathology.
Sound Engineering at CPCC: What You Need to Know
You may want to see also
Explore related products






![]()
Valvular Lesions: Correlating heart sounds with specific valve diseases
Valvular lesions are a critical area of focus in the USMLE, particularly when it comes to correlating heart sounds with specific valve diseases. Understanding these correlations is essential for diagnosing and managing patients with valvular heart disease. Heart sounds provide valuable clues about the function and integrity of the heart valves, and recognizing abnormal sounds can guide further diagnostic workup. For instance, aortic stenosis is characterized by a harsh, crescendo-decrescendo murmur best heard at the right second intercostal space. This murmur occurs during systole and is often accompanied by a delayed or soft S2, reflecting the obstruction to blood flow from the left ventricle into the aorta.
Mitral regurgitation, another common valvular lesion, presents with a holosystolic murmur heard best at the apex with the patient in the left lateral decubitus position. This murmur is due to the backflow of blood from the left ventricle into the left atrium during systole. A key distinguishing feature is the presence of a third heart sound (S3), which indicates volume overload in the left ventricle. In contrast, mitral stenosis produces a low-pitched diastolic rumble, best heard at the apex with the patient in the left lateral decubitus position and with the bell of the stethoscope. This murmur reflects the obstruction to blood flow from the left atrium into the left ventricle during diastole.
Tricuspid regurgitation is often associated with right-sided heart failure or pulmonary hypertension and manifests as a holosystolic murmur heard best at the left lower sternal border. This murmur is typically softer than that of mitral regurgitation but can be accentuated by inspiration (Carvallo’s sign). Pulmonic stenosis, though less common, presents with a high-pitched, crescendo-decrescendo systolic murmur heard at the left second intercostal space, similar to aortic stenosis but with a narrower focus and without the delayed S2.
Correlating these heart sounds with specific valve diseases requires a systematic approach to the cardiac exam. The timing, quality, duration, and location of murmurs are critical in distinguishing between lesions. For example, a systolic murmur does not always indicate regurgitation; it could also signify stenosis, as in the case of aortic or pulmonic stenosis. Similarly, diastolic murmurs are not exclusive to regurgitation but can also indicate stenosis, as seen in mitral stenosis. Mastery of these correlations is vital for the USMLE, as questions often test the ability to diagnose valvular lesions based on clinical findings, including heart sounds.
In summary, valvular lesions produce distinct heart sounds that are key to their diagnosis. Aortic stenosis and pulmonic stenosis share a systolic ejection murmur but differ in location and associated findings. Mitral regurgitation and tricuspid regurgitation both present with holosystolic murmurs but are distinguished by their location and clinical context. Mitral stenosis is unique with its diastolic rumble. Recognizing these patterns and understanding their pathophysiological basis is crucial for success on the USMLE and in clinical practice. Practice with auscultation and correlating findings with valve diseases will reinforce this knowledge and improve diagnostic accuracy.
Discover the Healing Power of Sound Frequencies for Wellness
You may want to see also
Explore related products





![]()
Exam Techniques: Proper auscultation methods and common USMLE case scenarios
Mastering auscultation is crucial for the USMLE, as heart sounds and murmurs are frequently tested in both Step 1 and Step 2. Proper technique ensures accurate identification of normal and abnormal findings. Begin by ensuring the patient is in a comfortable position, either sitting upright or lying supine. Use the bell of the stethoscope for low-pitched sounds (S1, S3, murmurs) and the diaphragm for high-pitched sounds (S2, splits, clicks). Place the stethoscope lightly on the skin to avoid artifactual noises. The four main auscultation areas for heart sounds are the mitral (apex), tricuspid, pulmonary, and aortic areas. Familiarize yourself with their anatomical locations to avoid missing key findings during the exam.
When auscultating, start by identifying the first and second heart sounds (S1 and S2). S1 is low-pitched and corresponds to mitral and tricuspid valve closure, while S2 is higher-pitched and represents aortic and pulmonary valve closure. Listen for extra heart sounds like S3 (ventricular filling) or S4 (atrial contraction), which are pathognomonic for specific conditions. Murmurs are another critical component; note their timing (systolic vs. diastolic), grade (1-6), location, radiation, and quality (e.g., harsh, blowing). For example, a systolic ejection murmur at the left sternal border suggests aortic stenosis, while a diastolic murmur at the apex points to mitral stenosis. Practice correlating murmurs with their associated hemodynamics and pathophysiology.
Common USMLE case scenarios often test auscultation findings in the context of clinical vignettes. For instance, a patient with dyspnea, paroxysmal nocturnal dyspnea, and a loud S1 may have mitral stenosis. Another scenario could involve a child with a systolic murmur, a palpable thrill, and a widened pulse pressure, suggesting patent ductus arteriosus. In these cases, the examiner will expect you to describe the auscultation findings accurately and relate them to the diagnosis. Be prepared to explain the mechanism behind the murmur, such as turbulent blood flow across a stenotic valve or a left-to-right shunt.
During the exam, approach auscultation systematically. Always listen to all four valve areas and note any splits in S2, which can indicate conditions like right bundle branch block or pulmonary hypertension. If a murmur is present, characterize it thoroughly and consider its clinical implications. For example, a holosystolic murmur at the apex that radiates to the axilla is classic for mitral regurgitation. Practice with recordings or simulators to train your ear to recognize these sounds, as the USMLE may include audio-based questions.
Finally, integrate auscultation findings with other clinical data. For instance, a patient with fever, a new heart murmur, and janeway lesions likely has infective endocarditis. Understanding how auscultation fits into the broader clinical picture is essential for answering USMLE questions correctly. Review common conditions associated with specific heart sounds and murmurs, such as aortic regurgitation (high-pitched, early diastolic murmur at the left sternal border) or hypertrophic cardiomyopathy (loud S4 and a dynamic left ventricular outflow tract murmur). By combining proper technique with clinical correlation, you’ll be well-prepared to tackle auscultation-related questions on the USMLE.
Overdrive Sound: A Musical Speedster's Delight
You may want to see also
Frequently asked questions
Yes, heart sounds are a common topic on the USMLE Step 1, particularly in the context of cardiovascular auscultation and pathophysiology.
Focus on normal heart sounds (S1 and S2), extra heart sounds (S3 and S4), murmurs (systolic and diastolic), and their clinical significance.
While hands-on auscultation is not tested, you should understand the characteristics of heart sounds, their locations, and their association with specific conditions.
Yes, heart murmurs are high-yield. Understand their timing (systolic vs. diastolic), intensity (grade), and associated conditions like valvular disease.
While rare, some questions may include audio clips or descriptions of heart sounds. Focus on recognizing patterns and clinical correlations.