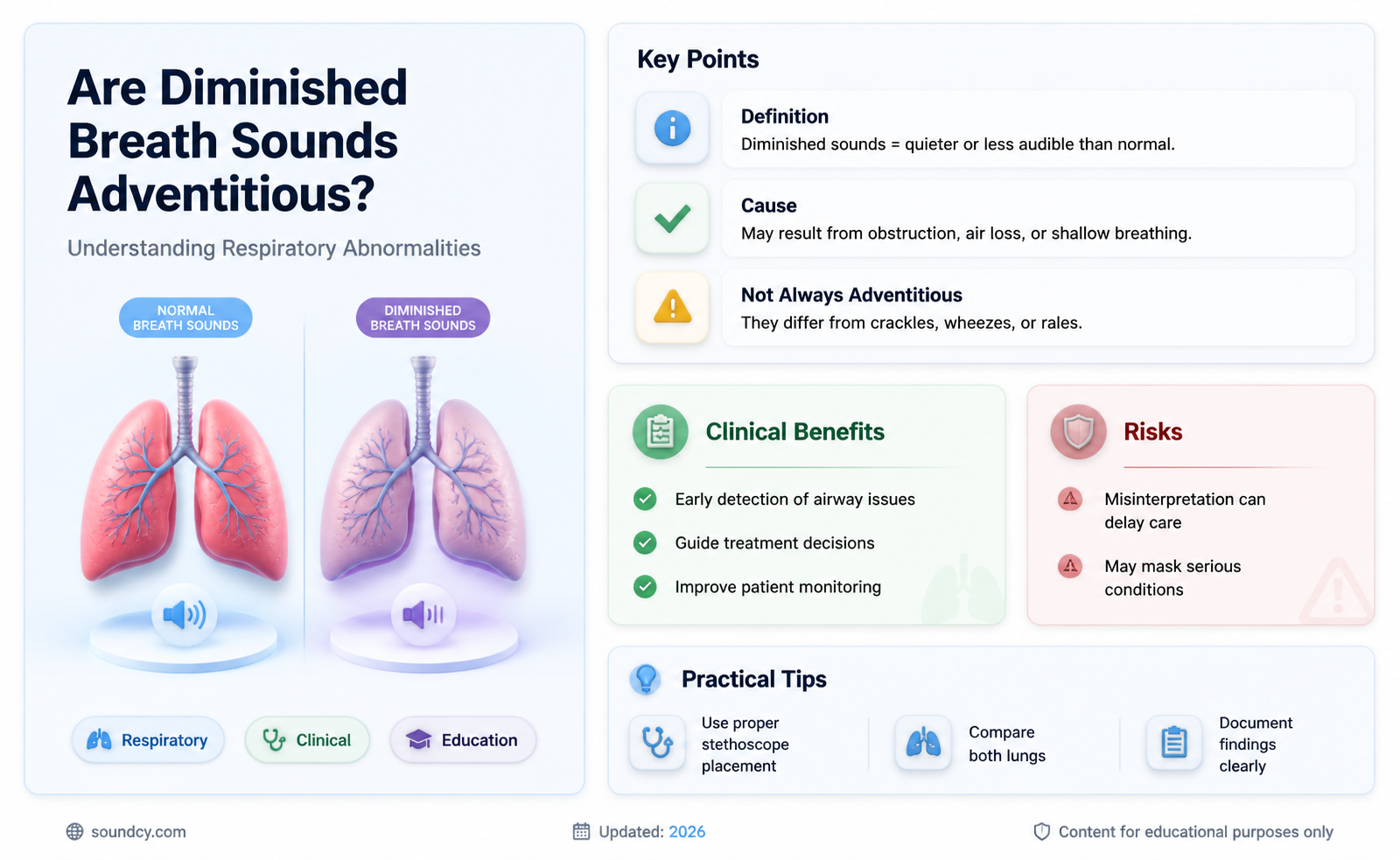
Diminished breath sounds, characterized by reduced or absent airflow during auscultation, are often a clinical concern, but their classification as adventitious remains a subject of debate. Adventitious sounds typically refer to abnormal, added lung sounds such as crackles, wheezes, or rhonchi, whereas diminished breath sounds imply a decrease in normal airflow. While diminished breath sounds can result from conditions like pneumothorax, consolidation, or airway obstruction, they are not inherently adventitious, as they do not represent an additional or abnormal sound. Instead, they reflect a reduction in the expected respiratory sounds. Understanding this distinction is crucial for accurate diagnosis and management, as it guides clinicians in identifying the underlying cause and differentiating between conditions that alter lung sound intensity versus those that introduce new, abnormal sounds.
| Characteristics | Values |
|---|---|
| Definition | Diminished breath sounds refer to reduced or decreased intensity of lung sounds during auscultation. |
| Adventitious | Diminished breath sounds are not considered adventitious. Adventitious sounds are added sounds (e.g., wheezes, crackles, rhonchi), whereas diminished sounds indicate a reduction in normal breath sounds. |
| Causes | Obstruction (e.g., COPD, asthma), consolidation (e.g., pneumonia), pleural effusion, pneumothorax, or reduced air entry due to poor effort or obesity. |
| Location | Can occur unilaterally or bilaterally, depending on the underlying cause. |
| Clinical Significance | May indicate airway obstruction, parenchymal lung disease, or pleural abnormalities. Requires further evaluation. |
| Differential Diagnosis | Distinguish from normal breath sounds; compare with contralateral side for asymmetry. |
| Associated Findings | May be accompanied by tachypnea, hypoxia, or other signs of respiratory distress. |
| Diagnostic Tools | Auscultation with a stethoscope; may require imaging (X-ray, CT) or pulmonary function tests for confirmation. |
| Treatment | Address underlying cause (e.g., bronchodilators for COPD, antibiotics for pneumonia, drainage for pleural effusion). |
| Prognosis | Depends on the cause; reversible if underlying condition is treated effectively. |
Explore related products






What You'll Learn
- Causes of Diminished Breath Sounds (e.g., pneumonia, atelectasis, pleural effusion, obesity, muscle weakness)
- Adventitious Sounds vs. Diminished Sounds (crackles, wheezes, rhonchi are adventitious, not diminished)
- Assessment Techniques (auscultation, comparison of lung fields, patient positioning)
- Clinical Significance (indicates airway obstruction, consolidation, or reduced air entry)
- Differential Diagnosis (COPD, pneumothorax, fibrosis, foreign body, neuromuscular disorders)
![]()
Causes of Diminished Breath Sounds (e.g., pneumonia, atelectasis, pleural effusion, obesity, muscle weakness)
Diminished breath sounds, also known as decreased or reduced breath sounds, occur when the normal air movement in the lungs is obstructed or restricted, leading to quieter or absent lung sounds upon auscultation. This condition is not considered adventitious, as adventitious sounds refer to abnormal sounds added to the breath cycle, such as crackles or wheezes. Instead, diminished breath sounds indicate an underlying issue affecting airflow or lung tissue. Understanding the causes of diminished breath sounds is crucial for accurate diagnosis and management. Below are several key conditions that can lead to this clinical finding.
Pneumonia is a common cause of diminished breath sounds. This infection inflames the air sacs in one or both lungs, often filling them with fluid or pus. The consolidation of lung tissue in pneumonia reduces the space available for air movement, leading to decreased breath sounds in the affected area. Additionally, the inflammation and fluid accumulation can impair the transmission of sound, further contributing to the diminished auscultatory findings. Pneumonia can be caused by bacteria, viruses, or fungi, and its severity can vary widely, from mild to life-threatening.
Atelectasis, another significant cause, occurs when a portion of the lung collapses or does not inflate completely. This condition reduces the volume of the lung and limits air entry, resulting in diminished or absent breath sounds over the affected area. Atelectasis can be caused by various factors, including airway obstruction (e.g., mucus plugs, tumors, or foreign bodies), compression from external structures (e.g., pleural effusion or tumors), or surfactant deficiency. It is commonly seen postoperatively, in patients with respiratory distress, or in those who are bedridden and unable to take deep breaths.
Pleural effusion, the accumulation of fluid in the pleural space between the lung and chest wall, can also lead to diminished breath sounds. The fluid acts as a barrier, reducing the transmission of air and sound through the lung tissue. As the effusion increases in size, it can compress the underlying lung, further diminishing breath sounds in the affected area. Pleural effusions can result from various conditions, including heart failure, infection, cancer, or liver disease. The presence of a large effusion may also cause dullness to percussion and shifted respiratory landmarks upon physical examination.
Obesity is a systemic condition that can contribute to diminished breath sounds due to its mechanical effects on the chest wall and lungs. Excess adipose tissue in the thoracic and abdominal regions can restrict diaphragmatic movement and decrease lung compliance, leading to reduced tidal volumes and airflow. This limitation in lung expansion results in quieter breath sounds, particularly at the lung bases. Additionally, obesity is often associated with hypoventilation and increased work of breathing, which can exacerbate the reduction in breath sounds. Obese individuals may also have underlying conditions, such as obstructive sleep apnea, that further compromise respiratory function.
Muscle weakness, particularly involving the respiratory muscles like the diaphragm and intercostal muscles, can significantly reduce breath sounds. Conditions such as muscular dystrophy, myasthenia gravis, or prolonged immobilization can lead to atrophy or dysfunction of these muscles, impairing their ability to generate adequate airflow. Weak respiratory muscles result in shallow breathing and decreased lung volumes, which are reflected in diminished breath sounds upon auscultation. Patients with muscle weakness may also experience fatigue and shortness of breath, further limiting their ability to take deep breaths and produce normal breath sounds.
In summary, diminished breath sounds are a clinical sign of reduced airflow or lung tissue involvement, stemming from conditions such as pneumonia, atelectasis, pleural effusion, obesity, or muscle weakness. Each of these causes has distinct mechanisms that impair normal respiratory function, leading to the characteristic decrease in auscultatory findings. Recognizing these underlying conditions is essential for appropriate diagnostic evaluation and targeted treatment, ensuring optimal patient outcomes.
Transistor Radios: Music to Your Ears?
You may want to see also
Explore related products






![]()
Adventitious Sounds vs. Diminished Sounds (crackles, wheezes, rhonchi are adventitious, not diminished)
When assessing respiratory sounds, it is crucial to differentiate between adventitious sounds and diminished breath sounds, as they signify distinct underlying conditions. Adventitious sounds are abnormal, added lung sounds that should not be present in healthy individuals. These include crackles, wheezes, and rhonchi, which are often indicative of specific respiratory pathologies. For example, crackles are associated with fluid accumulation in the alveoli, wheezes suggest airway obstruction (e.g., asthma), and rhonchi indicate the presence of mucus or secretions in larger airways. These sounds are considered adventitious because they are not part of normal breath sounds and are always pathological.
In contrast, diminished breath sounds refer to a reduction in the intensity or volume of normal lung sounds, such as vesicular breathing. This occurs when air movement through the lungs is restricted or reduced, often due to conditions like pneumothorax, pneumonia, or severe obesity. Diminished breath sounds are not adventitious; they are a decrease in the expected normal sounds rather than the addition of abnormal ones. It is essential to recognize this distinction, as misclassifying diminished sounds as adventitious could lead to diagnostic confusion.
Clinicians must carefully auscultate the lungs to identify whether abnormal findings are adventitious sounds or diminished breath sounds. Adventitious sounds are typically localized and can be heard over specific areas of the lung, while diminished sounds are often more generalized. For instance, crackles may be heard in the lung bases in heart failure, whereas diminished sounds might be noted over an entire lung in a patient with a pneumothorax. Understanding this difference is critical for accurate diagnosis and treatment planning.
Another key point is that adventitious sounds are often described as "added" sounds, whereas diminished sounds are characterized by a "reduction" in normal sounds. This distinction helps in categorizing the findings correctly. For example, a patient with chronic obstructive pulmonary disease (COPD) may exhibit both wheezes (adventitious) and diminished breath sounds due to air trapping. Properly identifying and documenting these findings ensures a comprehensive assessment of respiratory function.
In summary, crackles, wheezes, and rhonchi are adventitious sounds, not diminished sounds. Adventitious sounds are abnormal additions to lung auscultation, while diminished sounds represent a decrease in normal breath sounds. Recognizing this difference is fundamental for accurate clinical evaluation and management of respiratory conditions. Clear differentiation between these two categories enhances diagnostic precision and guides appropriate therapeutic interventions.
How Shorty Headers Enhance Exhaust Sound: A Comprehensive Guide
You may want to see also
Explore related products






![]()
Assessment Techniques (auscultation, comparison of lung fields, patient positioning)
Assessment Techniques for Evaluating Diminished Breath Sounds
Auscultation is the cornerstone of assessing breath sounds and determining whether diminished sounds are adventitious or indicative of an underlying condition. Using a stethoscope, the clinician listens systematically to both lung fields, focusing on the quality and intensity of breath sounds. Normal breath sounds include bronchial, vesicular, and bronchovesicular sounds, each with distinct characteristics. Diminished breath sounds may present as reduced intensity or absence of these sounds in specific areas. During auscultation, the clinician should note any asymmetry between lung fields, as unilateral diminution often suggests localized pathology, such as pneumothorax, consolidation, or pleural effusion. Adventitious sounds, such as wheezes or crackles, are typically added sounds rather than diminished ones, but their presence can guide further evaluation of the underlying cause.
Comparison of lung fields is essential to differentiate between normal variation and abnormal findings. The clinician should auscultate both lungs symmetrically, comparing corresponding segments (e.g., right upper lobe to left upper lobe). Diminished breath sounds that are unilateral or localized suggest obstructive or restrictive processes, such as mucus plugging, atelectasis, or fibrosis. Bilateral diminution may indicate conditions like severe obesity, neuromuscular weakness, or interstitial lung disease. Additionally, comparing inspiratory and expiratory phases can provide clues; for example, prolonged expiratory phase with diminished sounds may suggest obstructive airway disease. This comparative approach ensures accuracy and helps distinguish between physiological variations and pathological changes.
Patient positioning plays a critical role in optimizing auscultation and assessing diminished breath sounds. The patient should be in a comfortable position, typically seated or supine, with the chest exposed. Posterior and lateral lung fields are best assessed with the patient seated and leaning slightly forward, while supine positioning allows for anterior and axillary auscultation. Encouraging the patient to take slow, deep breaths enhances the detection of subtle changes in breath sounds. In cases of suspected pleural effusion or pneumothorax, lateral decubitus positioning (affected side down) can help confirm the diagnosis by redistributing fluid or air. Proper positioning ensures comprehensive evaluation of all lung segments and minimizes artifacts that could obscure findings.
Incorporating these assessment techniques—auscultation, comparison of lung fields, and strategic patient positioning—allows clinicians to systematically evaluate diminished breath sounds. While diminished sounds are not typically classified as adventitious (which refers to added sounds like wheezes or crackles), their presence warrants careful consideration of underlying causes. By combining these methods, clinicians can differentiate between conditions such as airway obstruction, parenchymal disease, or pleural abnormalities, guiding appropriate diagnostic and therapeutic interventions. Mastery of these techniques is essential for accurate respiratory assessment and patient management.
Exploring the Musical Rhythms and Unique Cadence of an Italian Accent
You may want to see also
Explore related products






![]()
Clinical Significance (indicates airway obstruction, consolidation, or reduced air entry)
Diminished breath sounds, as opposed to adventitious sounds, hold significant clinical importance as they provide crucial insights into underlying respiratory conditions. When auscultating a patient's lungs, the absence or reduction of normal breath sounds can indicate several pathological processes, primarily related to airway obstruction, consolidation, or decreased air entry. These findings are essential for healthcare professionals to identify and manage respiratory disorders effectively.
Airway Obstruction: One of the key clinical implications of diminished breath sounds is the presence of an airway obstruction. This can occur due to various reasons, such as foreign body aspiration, tumors, or severe asthma attacks. In such cases, the airflow is restricted, leading to reduced breath sounds over the affected area. For instance, a complete obstruction may result in absent breath sounds, while partial obstruction could cause decreased intensity. Identifying these changes is vital for prompt intervention, as airway obstructions can be life-threatening and require immediate medical attention.
Consolidation: Another significant indicator is the presence of lung consolidation, commonly seen in pneumonia or pulmonary edema. When the lung tissue becomes consolidated, it loses its normal air-filled structure, leading to diminished or absent breath sounds. This is because the consolidated area cannot vibrate and produce the typical breath sounds. Healthcare providers should be vigilant in detecting these changes, as they may suggest an infectious or inflammatory process within the lungs, requiring appropriate treatment.
Reduced Air Entry: Diminished breath sounds can also signify reduced air entry into the lungs, which may be caused by conditions like chronic obstructive pulmonary disease (COPD), emphysema, or pneumothorax. In these cases, the lungs' ability to expand and fill with air is compromised, resulting in quieter or absent breath sounds. Assessing the extent and location of reduced air entry is crucial for diagnosing and monitoring the progression of such respiratory diseases.
Furthermore, the clinical significance lies in the differentiation between diminished breath sounds and adventitious sounds. While adventitious sounds like crackles or wheezes are added sounds, diminished breath sounds indicate a reduction or absence of normal respiratory sounds. This distinction is essential for accurate diagnosis and treatment planning. For instance, a patient with asthma may exhibit both wheezing (adventitious) and diminished breath sounds due to airway narrowing, providing valuable clues about the severity and nature of the condition.
In clinical practice, recognizing these subtle changes in breath sounds allows healthcare professionals to make informed decisions regarding patient management. It often prompts further investigations, such as imaging studies or pulmonary function tests, to confirm the suspected diagnosis. Early detection of airway obstruction, consolidation, or reduced air entry through auscultation can significantly impact patient outcomes, especially in critical care settings. Therefore, understanding the clinical significance of diminished breath sounds is a vital skill for medical practitioners in respiratory assessment and care.
Mastering the Art of Creating Realistic Eating Sounds for Content
You may want to see also
Explore related products






![]()
Differential Diagnosis (COPD, pneumothorax, fibrosis, foreign body, neuromuscular disorders)
Diminished breath sounds on auscultation can be a critical finding, often prompting a thorough differential diagnosis to identify the underlying cause. One of the primary conditions to consider is Chronic Obstructive Pulmonary Disease (COPD). COPD is characterized by airflow limitation due to chronic bronchitis or emphysema, leading to reduced air movement in the lungs. Patients with COPD often exhibit diminished breath sounds, particularly during expiration, due to airway obstruction and hyperinflation. A history of smoking, chronic cough, and progressive dyspnea are key clinical features. Spirometry confirming irreversible airflow obstruction is essential for diagnosis, and management focuses on bronchodilators, inhaled corticosteroids, and pulmonary rehabilitation.
Another important differential is pneumothorax, a condition where air accumulates in the pleural space, leading to lung collapse. Diminished or absent breath sounds on the affected side are a hallmark finding. Pneumothorax can be spontaneous, traumatic, or secondary to underlying lung disease. Patients often present with sudden onset of chest pain and dyspnea. A chest X-ray or CT scan is diagnostic, and treatment ranges from observation for small pneumothoraces to needle aspiration or chest tube placement for larger or symptomatic cases.
Pulmonary fibrosis is a chronic interstitial lung disease characterized by scarring of lung tissue, which can also lead to diminished breath sounds. This condition typically presents with gradual onset of dyspnea, dry cough, and fine inspiratory crackles on auscultation, though breath sounds may become diminished in advanced stages due to reduced lung compliance. High-resolution CT (HRCT) of the chest often reveals reticular opacities and honeycombing. Diagnosis is confirmed through a combination of imaging, pulmonary function tests, and sometimes lung biopsy. Management includes antifibrotic medications and supportive care, such as oxygen therapy.
Foreign body aspiration is a critical condition, particularly in pediatric or elderly populations, that can cause localized diminished breath sounds. The obstruction of a bronchus by a foreign body leads to reduced air entry in the affected lung segment or lobe. Patients may present with acute onset of choking, cough, wheezing, or unilateral diminished breath sounds. A chest X-ray may show hyperinflation or atelectasis, but the diagnosis is often confirmed by bronchoscopy. Prompt removal of the foreign body is essential to prevent complications such as pneumonia or respiratory distress.
Lastly, neuromuscular disorders such as muscular dystrophy, amyotrophic lateral sclerosis (ALS), or myasthenia gravis can lead to diminished breath sounds due to weakened respiratory muscles. These conditions result in reduced chest wall movement and decreased lung volumes, manifesting as decreased air entry on auscultation. Patients often have a history of progressive muscle weakness, fatigue, and respiratory insufficiency. Pulmonary function tests typically show restrictive physiology, and electromyography or other specialized tests may be needed to confirm the underlying neuromuscular disorder. Management focuses on supportive care, including non-invasive ventilation and respiratory muscle training.
In summary, diminished breath sounds are not adventitious but rather a key clinical sign that necessitates a broad differential diagnosis. Conditions such as COPD, pneumothorax, pulmonary fibrosis, foreign body aspiration, and neuromuscular disorders must be considered based on clinical presentation, imaging, and diagnostic testing. Accurate diagnosis is crucial for initiating appropriate management and improving patient outcomes.
Unlock Spotify Sound Capsule: A Step-by-Step Access Guide
You may want to see also
Frequently asked questions
No, diminished breath sounds are not adventitious. Adventitious sounds are abnormal, added sounds like crackles, wheezes, or rhonchi, whereas diminished breath sounds indicate a reduction in normal air movement.
Diminished breath sounds can result from conditions such as pneumothorax, pleural effusion, obesity, or consolidation of lung tissue, which reduce air entry into the lungs.
Diminished breath sounds are characterized by a decrease in the intensity of normal breath sounds, while adventitious sounds are additional, abnormal noises heard during inhalation or exhalation.
Yes, they can coexist. For example, a patient with pneumonia might have both diminished breath sounds due to consolidation and crackles (adventitious sounds) in the affected area.
Not always. Diminished breath sounds can be benign, such as in cases of obesity or poor inspiratory effort, but they can also indicate serious conditions like pneumothorax or pleural effusion, requiring further evaluation.