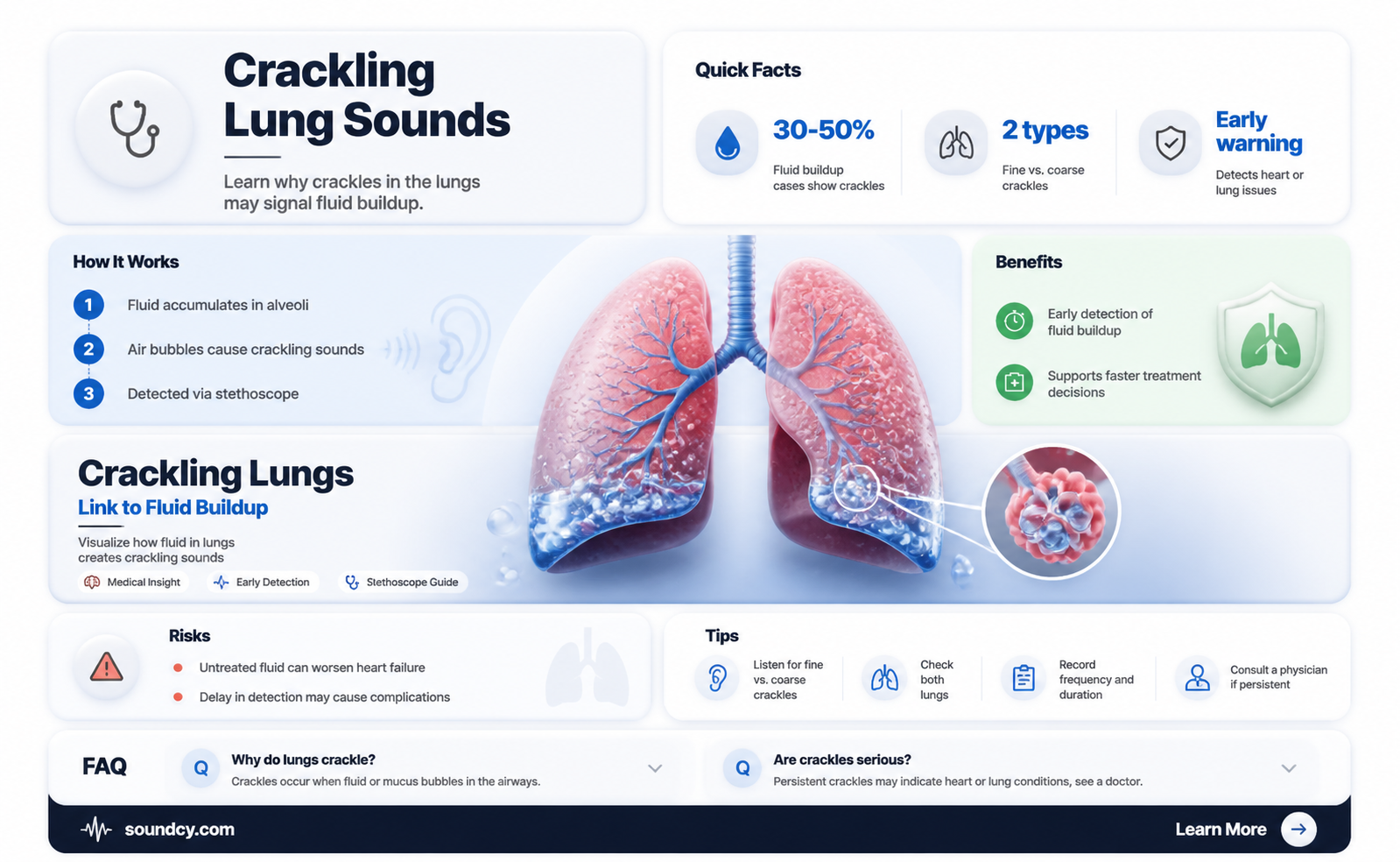
Crackling sounds, often described as fine or coarse rales, are abnormal lung sounds that can indicate the presence of fluid in the lungs, a condition known as pulmonary edema. These sounds occur when air passes through airways filled with fluid or mucus, creating a distinctive popping or bubbling noise during inhalation. Commonly heard during auscultation with a stethoscope, crackles are a key diagnostic indicator for various respiratory conditions, including pneumonia, heart failure, or acute respiratory distress syndrome (ARDS). Understanding the nature and causes of these sounds is crucial for healthcare professionals to accurately assess and manage underlying lung pathologies.
| Characteristics | Values |
|---|---|
| Medical Term | Crackles (also known as rales) |
| Cause | Fluid accumulation in the lungs (alveoli or small airways) |
| Associated Conditions | Pneumonia, heart failure, pulmonary edema, acute respiratory distress syndrome (ARDS), interstitial lung disease |
| Sound Description | High-pitched, bubbling, or rattling sounds during inhalation |
| Timing | Heard at the beginning or end of inspiration |
| Location | Typically basal (lower) lung fields, but can be diffuse |
| Severity | Varies from fine (soft) to coarse (loud), depending on fluid amount |
| Diagnosis | Auscultation with a stethoscope, confirmed by chest X-ray or CT scan |
| Treatment | Address underlying cause (e.g., diuretics for heart failure, antibiotics for pneumonia) |
| Prognosis | Depends on the underlying condition and timely intervention |
| Differential Diagnosis | Bronchitis, asthma, chronic obstructive pulmonary disease (COPD) |
| Prevalence | Common in patients with congestive heart failure or acute lung injury |
| Risk Factors | Heart disease, kidney disease, infection, exposure to toxins |
Explore related products






What You'll Learn
- Crackles vs. Wheezes: Differentiating between crackles (fluid) and wheezes (airway constriction) in lung auscultation
- Bibasilar Crackles: Crackles heard at the lung bases, often linked to heart failure or pneumonia
- Fine vs. Coarse Crackles: Fine crackles suggest fibrosis; coarse crackles indicate fluid accumulation
- Causes of Crackles: Conditions like pneumonia, pulmonary edema, or bronchitis causing fluid-related sounds
- Diagnosis and Treatment: Using stethoscopes, X-rays, and addressing underlying causes to manage fluid in lungs
![]()
Crackles vs. Wheezes: Differentiating between crackles (fluid) and wheezes (airway constriction) in lung auscultation
Lung auscultation is a critical skill for healthcare providers, offering immediate insights into respiratory health. Two common sounds—crackles and wheezes—often dominate the auditory landscape, but they signal distinct underlying issues. Crackles, typically associated with fluid in the lungs, manifest as brief, popping noises during inhalation, akin to the sound of walking on fresh snow. Wheezes, on the other hand, are high-pitched, whistling sounds that occur during both inhalation and exhalation, indicative of airway constriction. Differentiating between these sounds is essential for accurate diagnosis and targeted treatment.
To distinguish crackles from wheezes, consider their timing and characteristics. Crackles are primarily inspiratory, arising as air moves past fluid-filled alveoli or airways. They are often described as fine or coarse, with fine crackles being softer and shorter, while coarse crackles are louder and more prolonged. Wheezes, however, are continuous and musical, resulting from narrowed airways due to conditions like asthma or chronic obstructive pulmonary disease (COPD). A stethoscope is the primary tool for this differentiation, but the clinician’s ear must be attuned to the nuances of pitch, duration, and phase of respiration.
Practical tips can enhance accuracy in auscultation. For crackles, focus on the lung bases, where fluid tends to accumulate, especially in patients with heart failure or pneumonia. For wheezes, listen across the chest, noting whether the sound is localized or widespread, which can suggest the extent of airway obstruction. Patient positioning matters too: sitting upright may accentuate wheezes, while lying down can make crackles more apparent. Encouraging deep breaths during auscultation can also amplify these sounds, aiding in their identification.
Misinterpretation of these sounds can lead to misdiagnosis. For instance, mistaking wheezes for crackles might result in unnecessary diuretic therapy, while overlooking wheezes could delay bronchodilator administration. Clinicians should correlate auscultatory findings with patient history, symptoms, and other diagnostic tools like chest X-rays or spirometry. For example, a patient with a history of asthma presenting with wheezes would benefit from an inhaled beta-agonist, whereas crackles in a patient with leg edema suggest diuretics for fluid management.
In summary, crackles and wheezes are distinct auditory markers of lung pathology. Crackles indicate fluid in the lungs, while wheezes signal airway constriction. Mastery of auscultation techniques, combined with clinical context, ensures accurate differentiation and appropriate intervention. Whether in a hospital, clinic, or emergency setting, this skill remains indispensable for respiratory care.
Exploring the Gentle World of Quiet Sounds and Their Impact
You may want to see also
Explore related products






![]()
Bibasilar Crackles: Crackles heard at the lung bases, often linked to heart failure or pneumonia
Bibasilar crackles are a distinctive sound that healthcare providers listen for during auscultation, the act of listening to the internal sounds of the body, typically using a stethoscope. These crackles, often described as fine, high-pitched rattling noises, are specifically heard at the lung bases, the lower regions of the lungs. They are a critical indicator of underlying health issues, particularly fluid accumulation in the lungs, a condition known as pulmonary edema. This phenomenon is not merely a benign finding; it often signals serious conditions such as heart failure or pneumonia, making early detection and intervention crucial.
Understanding the Mechanism
Bibasilar crackles occur when air moves through airways filled with fluid or mucus, creating turbulence that produces the characteristic crackling sound. In heart failure, the heart’s inability to pump blood efficiently leads to fluid backup in the lungs, a process known as congestive heart failure. In pneumonia, infection causes inflammation and fluid buildup in the alveoli, the tiny air sacs where gas exchange occurs. Both conditions result in the same audible clue: crackles at the lung bases. This sound is more prominent during inhalation and is often described as "fine" or "velcro-like," distinguishing it from coarser crackles associated with other conditions like chronic obstructive pulmonary disease (COPD).
Clinical Significance and Diagnosis
Identifying bibasilar crackles is a key diagnostic step in differentiating between various respiratory and cardiac conditions. For instance, in heart failure, crackles are typically bilateral and accompanied by symptoms like shortness of breath, fatigue, and leg swelling. In pneumonia, crackles may be localized to one lung base, often with fever, cough, and sputum production. Healthcare providers use this information, along with imaging studies like chest X-rays or CT scans, to confirm the presence of fluid and determine its cause. Early recognition of these crackles can lead to timely treatment, such as diuretics for heart failure or antibiotics for pneumonia, potentially preventing complications like respiratory distress or organ damage.
Practical Tips for Patients and Caregivers
For individuals at risk of heart failure or pneumonia, monitoring for symptoms like persistent cough, wheezing, or shortness of breath is essential. If bibasilar crackles are detected during a medical exam, patients should follow their provider’s recommendations closely. Lifestyle modifications, such as reducing salt intake to manage fluid retention in heart failure, or staying up-to-date on vaccinations like the pneumococcal vaccine to prevent pneumonia, can be proactive measures. Caregivers should also be vigilant, especially in older adults or those with chronic conditions, as they are more susceptible to these issues. Prompt medical attention at the first sign of respiratory distress can make a significant difference in outcomes.
Takeaway: A Sound That Demands Attention
Bibasilar crackles are more than just an auditory finding; they are a red flag for potentially life-threatening conditions. Whether stemming from heart failure or pneumonia, these crackles indicate fluid in the lungs, a situation that requires immediate medical evaluation. By understanding their significance and taking proactive steps, patients and healthcare providers can work together to address the underlying causes and improve long-term health. Listening closely to the body’s signals, quite literally in this case, can be the first step toward effective treatment and recovery.
Mastering Pronunciation: When 'U' Sounds Like 'Put' in English
You may want to see also
Explore related products






![]()
Fine vs. Coarse Crackles: Fine crackles suggest fibrosis; coarse crackles indicate fluid accumulation
Crackling sounds in the lungs, known as rales, are a critical diagnostic clue for healthcare providers. These sounds, heard through a stethoscope, can differentiate between fine and coarse crackles, each pointing to distinct underlying conditions. Fine crackles, often described as brief, high-pitched sounds resembling the rustling of hair or cellophane, are typically associated with fibrosis or scarring of lung tissue. In contrast, coarse crackles are louder, lower-pitched, and more bubbling, indicating fluid accumulation in the airways, such as in pneumonia or heart failure. Understanding this distinction is essential for accurate diagnosis and targeted treatment.
To identify fine crackles, clinicians listen for sounds that are short and discontinuous, often heard at the end of inhalation. These crackles are commonly found in interstitial lung diseases, such as idiopathic pulmonary fibrosis, where scarring reduces lung elasticity. Fine crackles may also be present in conditions like sarcoidosis or scleroderma, where inflammation and fibrosis affect the lung parenchyma. Early detection of these sounds can prompt further imaging, such as a high-resolution CT scan, to confirm the extent of fibrosis and guide management, which may include antifibrotic medications or pulmonary rehabilitation.
Coarse crackles, on the other hand, are more dramatic and easier to hear, often described as rattling or gurgling. They occur when larger airways are filled with mucus, pus, or fluid, as seen in acute conditions like bronchitis, pneumonia, or congestive heart failure. These crackles are typically heard at the beginning of inspiration and may be localized to specific lung regions. For instance, in left-sided heart failure, coarse crackles are often present at the lung bases due to pulmonary edema. Treatment focuses on addressing the underlying cause, such as diuretics for fluid overload or antibiotics for infection, with prompt intervention being key to preventing complications.
A practical tip for distinguishing between fine and coarse crackles is to compare them to everyday sounds: fine crackles resemble the crackling of snow underfoot, while coarse crackles are akin to pouring water into a glass. Additionally, patient positioning can enhance auscultation; for example, having the patient sit upright may accentuate crackles in lower lung fields. For healthcare providers, documenting the type, location, and timing of crackles is crucial for monitoring disease progression and treatment efficacy.
In summary, fine and coarse crackles serve as auditory markers of distinct pulmonary pathologies. Fine crackles signal fibrosis and interstitial lung disease, requiring long-term management strategies, while coarse crackles indicate acute fluid accumulation, often necessitating immediate intervention. By mastering the art of auscultation and understanding these nuances, clinicians can improve diagnostic accuracy and patient outcomes, ensuring that the right treatment is delivered at the right time.
Best Sound Devices to Pair with Focusrite for Optimal Audio Quality
You may want to see also
Explore related products






![]()
Causes of Crackles: Conditions like pneumonia, pulmonary edema, or bronchitis causing fluid-related sounds
Crackling sounds in the lungs, often described as rales, are a telltale sign of fluid accumulation in the airways or alveoli. These sounds occur when air moves through airways narrowed or partially blocked by fluid, mucus, or inflammation. While they can be benign and transient, persistent crackles often signal underlying conditions that require medical attention. Pneumonia, pulmonary edema, and bronchitis are among the most common culprits, each with distinct mechanisms that lead to fluid-related lung sounds.
Pneumonia, an infection of the lung tissue, causes crackles by triggering inflammation and fluid buildup in the alveoli. Bacterial, viral, or fungal pathogens invade the lungs, prompting the immune system to respond with mucus production and fluid leakage into the air sacs. This process not only impairs oxygen exchange but also creates the characteristic crackling sounds during inhalation. For instance, bacterial pneumonia often presents with fever, cough, and purulent sputum, while viral pneumonia may be accompanied by systemic symptoms like fatigue and muscle aches. Treatment typically involves antibiotics for bacterial cases, antiviral medications for viral infections, and supportive care such as hydration and oxygen therapy.
Pulmonary edema, a condition where excess fluid accumulates in the lungs, is another significant cause of crackles. This can result from heart failure, where the heart’s inability to pump blood effectively leads to fluid backup in the pulmonary circulation. Non-cardiogenic causes, such as acute respiratory distress syndrome (ARDS) or high-altitude pulmonary edema, also contribute to fluid buildup. Crackles in pulmonary edema are often described as fine and widespread, reflecting the diffuse nature of fluid distribution. Management focuses on addressing the underlying cause—diuretics for heart failure, positive pressure ventilation for ARDS, and supplemental oxygen for all cases.
Bronchitis, inflammation of the bronchial tubes, produces crackles when mucus secretion and airway swelling obstruct airflow. Acute bronchitis, often viral, typically resolves within weeks, while chronic bronchitis, a hallmark of COPD, persists due to long-term irritant exposure like smoking. Crackles in bronchitis are usually accompanied by wheezing and a productive cough. Treatment includes bronchodilators to relieve airway constriction, mucolytics to thin mucus, and, in chronic cases, pulmonary rehabilitation programs. Avoiding triggers like tobacco smoke and pollutants is crucial for prevention.
Understanding the specific cause of crackles is essential for targeted treatment. For example, a patient with pneumonia may require a 7- to 10-day course of amoxicillin (500 mg every 8 hours), while someone with heart-failure-induced pulmonary edema might benefit from furosemide (20–40 mg daily) to reduce fluid retention. In bronchitis, inhaled albuterol (90 mcg as needed) can provide quick relief. Early diagnosis through auscultation, imaging, and lab tests ensures appropriate intervention, preventing complications like respiratory failure or sepsis. Always consult a healthcare provider for personalized care, as self-management can delay critical treatment.
Master the Art of Creating Hilarious Sounds: Tips and Tricks
You may want to see also
Explore related products






![]()
Diagnosis and Treatment: Using stethoscopes, X-rays, and addressing underlying causes to manage fluid in lungs
Crackling sounds heard through a stethoscope, known as rales, often signal fluid accumulation in the lungs, a condition called pulmonary edema. These abnormal breath sounds occur when air moves through airways filled with fluid, creating a distinctive popping or bubbling noise. Identifying and addressing the underlying cause of this fluid buildup is critical for effective management.
Diagnosis begins with a thorough physical examination, where a healthcare provider uses a stethoscope to listen for rales, which may be fine or coarse depending on the extent and location of fluid. Fine crackles, heard at the end of inspiration, often indicate fluid in the small airways, while coarse crackles, audible during both inspiration and expiration, suggest larger airway involvement.
Imaging plays a pivotal role in confirming the presence and extent of pulmonary fluid. A chest X-ray is typically the first-line diagnostic tool, revealing a characteristic "butterfly" or "bat-wing" pattern of fluid accumulation in the lungs. For more detailed assessment, a CT scan may be employed to differentiate between pulmonary edema and other conditions like pneumonia or lung cancer. In some cases, an ultrasound can detect fluid in the pleural space, aiding in distinguishing between intra-pulmonary and extra-pulmonary fluid.
Treatment strategies focus on alleviating symptoms and addressing the root cause of fluid buildup. For acute cases, such as cardiogenic pulmonary edema due to heart failure, diuretics like furosemide (20–40 mg IV) are administered to reduce fluid volume. Oxygen therapy is often initiated to improve oxygenation, with a target SpO2 of 92–96% in most patients. In severe cases, non-invasive ventilation (NIV) or mechanical ventilation may be required to support breathing.
Chronic conditions contributing to pulmonary fluid, such as chronic obstructive pulmonary disease (COPD) or interstitial lung disease, necessitate long-term management. This includes bronchodilators, corticosteroids, and pulmonary rehabilitation programs tailored to the patient’s needs. For patients with recurrent pleural effusions, procedures like thoracentesis or pleurodesis may be performed to remove fluid and prevent reaccumulation.
Patient education and lifestyle modifications are integral to preventing recurrence. Encouraging adherence to prescribed medications, monitoring daily weights to detect early fluid retention, and adopting a low-sodium diet are practical steps for individuals with heart failure or kidney disease. Regular follow-ups with healthcare providers ensure timely adjustments to treatment plans, optimizing outcomes and quality of life. By combining diagnostic precision with targeted interventions, fluid in the lungs can be effectively managed, reducing morbidity and mortality.
Unveiling the Silent World: Do Worms Make Any Sounds?
You may want to see also
Frequently asked questions
Crackling sounds, also known as rales, are often caused by fluid, mucus, or pus in the small air sacs (alveoli) of the lungs, which can occur due to conditions like pneumonia, heart failure, or acute respiratory distress syndrome (ARDS).
While crackling sounds often indicate fluid in the lungs, they can also result from other conditions such as lung scarring, chronic obstructive pulmonary disease (COPD), or collapsed lung tissue.
Crackling sounds are typically diagnosed through a physical examination using a stethoscope. Additional tests like chest X-rays, CT scans, or ultrasounds may be used to confirm the presence of fluid or other underlying issues.
Treatment depends on the underlying cause. For fluid in the lungs, options may include diuretics (for heart failure), antibiotics (for infections), or oxygen therapy. Addressing the root cause is essential for effective management.
Seek immediate medical attention if crackling sounds are accompanied by severe shortness of breath, chest pain, coughing up blood, or bluish lips or skin, as these could indicate a serious condition requiring urgent care.