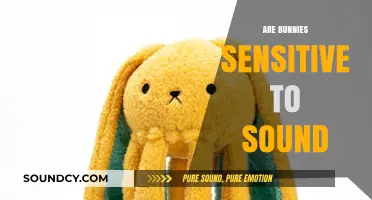
Bronchial breath sounds are a type of lung sound that can be heard during auscultation, typically over the trachea or large airways. While they are often associated with certain respiratory conditions, such as pneumonia or consolidation, their presence alone does not necessarily indicate an abnormality. In some cases, bronchial breath sounds can be heard in healthy individuals, particularly over the upper trachea or in specific anatomical locations. Understanding whether bronchial breath sounds are normal or indicative of an underlying issue requires careful consideration of their characteristics, location, and accompanying clinical context.
| Characteristics | Values |
|---|---|
| Location | Normally heard over the trachea and mainstem bronchi (e.g., suprasternal notch, upper back) |
| Intensity | Loud and high-pitched |
| Duration | Equal inspiratory and expiratory phases |
| Quality | Hollow, tubular, or "bark-like" sound |
| Normalcy | Not normal over lung fields; only normal over trachea and mainstem bronchi |
| Associated Conditions (if heard over lung fields) | Pneumonia, consolidation, asthma, COPD exacerbation, pulmonary edema, foreign body aspiration |
| Differential Diagnosis | Requires comparison with other breath sounds (e.g., vesicular, wheezes, crackles) |
| Clinical Significance | Abnormal if heard outside typical locations, indicating possible airway or parenchymal disease |
Explore related products






What You'll Learn
- Characteristics of Normal Bronchial Sounds: Clear, hollow, tubular sounds heard over trachea, larynx, and bronchi
- Abnormal Bronchial Breath Sounds: Include wheezing, rhonchi, stridor, indicating airway obstruction or inflammation
- Locations for Auscultation: Best heard over trachea, suprasternal notch, and main bronchi areas
- Comparison with Other Sounds: Differentiate from vesicular, crackles, and pleural friction rubs
- Clinical Significance: Normal sounds indicate healthy airways; abnormalities suggest conditions like COPD, asthma, or pneumonia
![]()
Characteristics of Normal Bronchial Sounds: Clear, hollow, tubular sounds heard over trachea, larynx, and bronchi
Normal bronchial breath sounds are a fundamental aspect of respiratory assessment, providing valuable insights into the health of the airways. These sounds are characterized by their clear, hollow, and tubular qualities, which are typically heard over the trachea, larynx, and bronchi. When auscultating these areas, healthcare professionals listen for these distinct sounds to ensure the airways are functioning optimally. The clarity of bronchial sounds indicates unobstructed airflow, while their hollow and tubular nature reflects the anatomical structure of the larger airways. These characteristics are essential for differentiating normal sounds from abnormal ones, such as wheezes or crackles, which may signify underlying respiratory conditions.
The location of bronchial breath sounds is a critical factor in their assessment. They are most prominently heard over the trachea, larynx, and main bronchi, where the airways are largest and most direct. The sound intensity is typically louder in these areas due to the proximity of the stethoscope to the air columns. It is important to note that bronchial sounds should not be heard in peripheral lung fields, as this could indicate consolidation or other pathological processes. Proper auscultation technique, including correct placement of the stethoscope and patient positioning, is crucial for accurately identifying these sounds.
The quality of normal bronchial sounds is another distinguishing feature. They are described as hollow and tubular, resembling the sound of breathing through a pipe or tube. This quality arises from the airflow moving through the larger, more rigid airways. Unlike vesicular breath sounds, which are softer and heard in the smaller bronchioles and alveoli, bronchial sounds are more intense and higher-pitched. The clarity of these sounds is paramount; any muffling or distortion could suggest the presence of mucus, inflammation, or other obstructions in the airways.
Intensity and pitch are additional characteristics of normal bronchial sounds. They are generally louder and higher-pitched compared to other lung sounds due to the larger diameter of the airways. The intensity may vary slightly with inspiration and expiration, but it remains relatively consistent throughout the respiratory cycle. Assessing these aspects helps differentiate bronchial sounds from other sounds, such as adventitious breath sounds, which may be intermittent or vary in intensity.
In summary, normal bronchial breath sounds are clear, hollow, and tubular and are heard primarily over the trachea, larynx, and bronchi. Their distinct qualities, including location, intensity, pitch, and clarity, are essential for accurate respiratory assessment. Understanding these characteristics enables healthcare providers to identify deviations from normal, facilitating early detection and management of respiratory conditions. Mastery of auscultation techniques and familiarity with these sounds are indispensable skills for any clinician involved in respiratory care.
Discover the Unique and Enchanting Sounds of Mockingbirds
You may want to see also
Explore related products

$12.99





![]()
Abnormal Bronchial Breath Sounds: Include wheezing, rhonchi, stridor, indicating airway obstruction or inflammation
Abnormal bronchial breath sounds are indicative of underlying respiratory issues, often pointing to airway obstruction or inflammation. These sounds, which include wheezing, rhonchi, and stridor, are distinct from normal bronchial breath sounds, which are typically clear and quiet during both inspiration and expiration. Recognizing these abnormal sounds is crucial for healthcare providers to diagnose and manage respiratory conditions effectively. Each of these sounds has unique characteristics and is associated with specific pathophysiological processes.
Wheezing is a high-pitched, whistling sound that occurs primarily during expiration but can also be heard during inspiration in severe cases. It is caused by the narrowing of airways due to inflammation, mucus plugging, or bronchospasm. Conditions such as asthma, chronic obstructive pulmonary disease (COPD), and bronchitis commonly produce wheezing. The sound is generated by turbulent airflow through partially obstructed airways. Wheezing is often described as musical and can vary in intensity depending on the degree of airway constriction. Early identification of wheezing is essential, as it may indicate acute exacerbations of chronic conditions or the need for immediate intervention, such as bronchodilators.
Rhonchi are low-pitched, rattling sounds that resemble snoring and are typically heard during inspiration, though they can also occur during expiration. Unlike wheezing, rhonchi are often associated with the presence of mucus or secretions in the larger airways. Conditions such as pneumonia, chronic bronchitis, and cystic fibrosis frequently produce rhonchi. These sounds are caused by air moving past mucus or other obstructions in the bronchial tree. Clearing these secretions through techniques like chest physiotherapy or suctioning can often alleviate rhonchi. Persistent rhonchi may indicate inadequate mucus clearance or ongoing infection, requiring further evaluation and treatment.
Stridor is a high-pitched, harsh sound that is usually heard during inspiration and is indicative of upper airway obstruction. Unlike wheezing and rhonchi, which originate in the lower airways, stridor is caused by narrowing or blockage in the larynx, trachea, or large bronchi. Conditions such as croup, epiglottitis, foreign body aspiration, or tumors can produce stridor. The sound is often described as musical but is more intense and alarming than wheezing. Stridor is a medical emergency, as it can rapidly progress to complete airway obstruction. Immediate assessment and intervention, such as securing the airway or administering medications to reduce swelling, are critical in managing stridor.
In summary, abnormal bronchial breath sounds like wheezing, rhonchi, and stridor are important clinical indicators of airway obstruction or inflammation. Wheezing and rhonchi are typically associated with lower airway issues, while stridor signals upper airway compromise. Each sound has distinct characteristics that help differentiate the underlying cause. Healthcare providers must be adept at recognizing these sounds to initiate appropriate diagnostic and therapeutic measures. Early detection and management of these abnormal breath sounds can significantly improve patient outcomes and prevent complications related to respiratory distress.
How Autistic People Experience Sound Differently
You may want to see also
Explore related products






![]()
Locations for Auscultation: Best heard over trachea, suprasternal notch, and main bronchi areas
Bronchial breath sounds are typically considered normal when auscultated over specific anatomical locations, primarily the trachea, suprasternal notch, and main bronchi areas. These locations are ideal for detecting bronchial breath sounds because they are closest to the larger airways where these sounds originate. The trachea, being the primary airway connecting the pharynx to the lungs, is a key area for auscultation. Placing the stethoscope directly over the trachea allows healthcare providers to hear the characteristic high-pitched, hollow sounds that are typical of bronchial breathing. This is because the trachea is a large airway where air movement is more turbulent, producing sounds that are easier to distinguish from other lung sounds.
The suprasternal notch, located at the base of the neck just above the sternum, is another optimal location for auscultating bronchial breath sounds. This area is particularly useful because it is directly aligned with the trachea and the upper part of the bronchial tree. When listening here, the sounds are often clearer and more pronounced, especially in individuals with normal lung function. The suprasternal notch is also easily accessible, making it a practical site for routine auscultation. It is important to ensure proper placement of the stethoscope to avoid picking up artifacts from surrounding tissues or clothing.
The main bronchi areas, specifically the right and left main bronchi, are additional locations where bronchial breath sounds are best heard. The right main bronchus is wider, shorter, and more vertical than the left, which influences the intensity and quality of the sounds heard. Auscultation over these areas requires careful positioning of the stethoscope to capture the sounds emanating from the larger airways. For the right main bronchus, the stethoscope is typically placed over the sternal border in the second to fourth intercostal spaces, while for the left main bronchus, it is placed slightly lower and more laterally. These positions ensure that the stethoscope is directly over the bifurcation of the trachea and the main bronchi, where bronchial breath sounds are most prominent.
When auscultating these locations, it is crucial to differentiate bronchial breath sounds from other lung sounds, such as vesicular or adventitious sounds. Bronchial breath sounds are characterized by their high-pitched, hollow quality and are normally heard only over the trachea and main bronchi. If these sounds are heard in other lung fields, it may indicate consolidation or other pathological conditions. Therefore, understanding the normal auscultation locations helps in accurately assessing lung health and identifying abnormalities.
In summary, the trachea, suprasternal notch, and main bronchi areas are the best locations for auscultating bronchial breath sounds. These sites are chosen because they are closest to the larger airways where these sounds originate, ensuring clarity and accuracy in assessment. Proper placement of the stethoscope over these areas is essential for distinguishing normal bronchial breath sounds from other lung sounds and for detecting any deviations that may indicate underlying respiratory issues. Mastery of these auscultation techniques is fundamental for healthcare providers in evaluating respiratory function and diagnosing lung conditions.
Control External Sound Modules via USB: A Guide
You may want to see also
Explore related products





![]()
Comparison with Other Sounds: Differentiate from vesicular, crackles, and pleural friction rubs
Bronchial breath sounds are a distinct type of lung sound that can be heard during auscultation, typically over the trachea or large airways. To understand their normalcy, it's essential to compare them with other common lung sounds, such as vesicular breath sounds, crackles, and pleural friction rubs. Vesicular breath sounds are the soft, low-pitched sounds heard over most of the lung fields during normal breathing. They are characterized by a longer inspiratory phase compared to the expiratory phase and are considered the standard for healthy lung function. In contrast, bronchial breath sounds are louder, higher-pitched, and have nearly equal inspiratory and expiratory durations. This distinction is crucial, as bronchial breath sounds over peripheral lung areas may indicate consolidation or fluid in the lungs, whereas they are normal over the trachea.
When differentiating bronchial breath sounds from crackles, it’s important to note that crackles are discontinuous, brief, popping sounds that occur due to the sudden opening of small airways filled with fluid, mucus, or secretions. Crackles are often heard in conditions like pneumonia, heart failure, or chronic obstructive pulmonary disease (COPD). Unlike the continuous and hollow quality of bronchial breath sounds, crackles are intermittent and can be fine or coarse, depending on the underlying cause. Auscultating for the presence of crackles alongside bronchial breath sounds can help clinicians localize the pathology and determine its severity.
Pleural friction rubs are another sound often compared with bronchial breath sounds. These are harsh, grating sounds that occur when inflamed pleural surfaces rub against each other during breathing. Pleural friction rubs are typically heard in conditions like pleurisy or pulmonary embolism. Unlike bronchial breath sounds, which are airway-related, pleural friction rubs are pleura-related and are characterized by their three-phase nature (inspiratory, expiratory, and sometimes during pauses in breathing). Recognizing this distinction is vital, as mistaking a pleural friction rub for a bronchial breath sound could lead to misdiagnosis.
In summary, while bronchial breath sounds are normal over the trachea, their presence in other lung areas may signify pathology. Vesicular breath sounds, with their softer and longer inspiratory phase, represent healthy lung function, whereas bronchial breath sounds are louder and more balanced. Crackles, with their discontinuous and popping nature, indicate airway obstruction or fluid, and pleural friction rubs, with their grating quality, point to pleural inflammation. Accurate differentiation of these sounds is essential for proper diagnosis and management of respiratory conditions.
Lastly, it’s instructive to practice auscultation systematically, comparing sounds across different lung fields and patient positions. For instance, asking the patient to breathe deeply and listening for changes in sound intensity or quality can help distinguish between bronchial breath sounds and other abnormalities. Mastery of these distinctions ensures that clinicians can interpret lung sounds accurately, leading to better patient outcomes. Understanding the nuances of these sounds is a cornerstone of respiratory assessment and underscores the importance of thorough physical examination in clinical practice.
Unraveling the Mysteries of Human Sound Perception and Processing
You may want to see also
Explore related products






![]()
Clinical Significance: Normal sounds indicate healthy airways; abnormalities suggest conditions like COPD, asthma, or pneumonia
Bronchial breath sounds are an essential component of respiratory assessment, providing valuable insights into the health of the airways. Normal bronchial breath sounds are typically heard over the trachea and mainstem bronchi, characterized by a hollow, tubular quality. These sounds indicate that air is moving freely through the larger airways, which is a sign of healthy respiratory function. Clinically, the presence of normal bronchial breath sounds reassures healthcare providers that the airways are patent and unobstructed, allowing for efficient gas exchange. This is particularly important in routine examinations and in monitoring patients with no known respiratory issues.
The clinical significance of normal bronchial breath sounds extends beyond mere reassurance. It serves as a baseline for comparison when abnormalities are detected. For instance, normal sounds indicate that the airways are free from inflammation, mucus plugging, or structural abnormalities. This is crucial because deviations from normal can signal underlying conditions. Abnormal bronchial breath sounds, such as wheezing, rhonchi, or stridor, often suggest the presence of diseases like chronic obstructive pulmonary disease (COPD), asthma, or pneumonia. Recognizing the difference between normal and abnormal sounds is therefore fundamental in early diagnosis and intervention.
In patients with COPD, bronchial breath sounds may be accompanied by wheezing or rhonchi due to airway narrowing and mucus accumulation. Asthma often presents with high-pitched wheezing, especially during exacerbations, as a result of bronchial constriction and inflammation. Pneumonia, on the other hand, may produce amplified bronchial breath sounds or crackles due to consolidation and increased airway secretions. Thus, the absence of normal bronchial breath sounds in these contexts is a critical indicator of pathology, guiding further diagnostic and therapeutic decisions.
Healthcare providers must be adept at auscultating bronchial breath sounds to interpret their clinical significance accurately. Normal sounds not only confirm healthy airways but also help rule out acute respiratory distress. Conversely, abnormalities prompt a deeper investigation into the patient’s history, symptoms, and additional diagnostic tests such as chest X-rays or pulmonary function tests. This proactive approach ensures timely management of conditions like COPD, asthma, or pneumonia, which can significantly impact patient outcomes if left untreated.
In summary, the clinical significance of bronchial breath sounds lies in their ability to reflect airway health. Normal sounds are indicative of unobstructed, functional airways, while abnormalities serve as red flags for conditions such as COPD, asthma, or pneumonia. Mastery of auscultation techniques and understanding the implications of these sounds are essential skills for healthcare professionals, enabling them to provide effective care and improve patient respiratory health.
Understanding the Heart's Lub Dub: How Cardiac Sounds Are Produced
You may want to see also
Frequently asked questions
Bronchial breath sounds are typically heard over the trachea but can be abnormal when heard over other lung areas. They may indicate conditions like pneumonia, consolidation, or lung cancer.
Normal bronchial breath sounds are loud, high-pitched, and hollow, often described as "tubular." They are usually heard over the trachea and main bronchi but should not be present in peripheral lung fields.
If bronchial breath sounds are heard outside the tracheal area, especially unilaterally or in peripheral lung fields, it may suggest an underlying issue such as infection, inflammation, or tissue consolidation, and medical evaluation is recommended.