Breath sounds and lung sounds are terms often used interchangeably in medical discussions, but understanding whether they are truly the same is essential for accurate clinical assessment. Both refer to the audible noises produced during the respiratory cycle, which can provide valuable insights into lung function and potential abnormalities. However, while breath sounds encompass all noises generated by air moving through the respiratory tract, lung sounds specifically focus on the sounds originating from the lungs themselves. This distinction is crucial because it highlights the need to differentiate between normal and abnormal auditory cues, ensuring proper diagnosis and treatment of respiratory conditions.
| Characteristics | Values |
|---|---|
| Definition | Breath sounds and lung sounds are often used interchangeably, referring to the sounds produced during inhalation and exhalation, which are auscultated using a stethoscope. |
| Origin | Both originate from the movement of air through the respiratory tract, including the trachea, bronchi, and alveoli. |
| Types | Include normal sounds (vesicular, bronchial, bronchovesicular) and abnormal sounds (wheezes, rhonchi, crackles, stridor). |
| Purpose | Used to assess lung health, diagnose respiratory conditions, and monitor treatment effectiveness. |
| Distinction | No clinical distinction; "breath sounds" and "lung sounds" are synonymous in medical practice. |
| Auscultation | Performed using a stethoscope over specific lung fields to evaluate sound quality, intensity, and duration. |
| Clinical Relevance | Essential for identifying conditions like asthma, pneumonia, COPD, and pulmonary edema. |
| Normal vs. Abnormal | Normal sounds are consistent with healthy lung function; abnormal sounds indicate pathology. |
| Subjectivity | Interpretation can vary slightly among healthcare providers but follows standardized guidelines. |
| Documentation | Both terms are used interchangeably in medical records and literature without differentiation. |
Explore related products






What You'll Learn
- Definition Comparison: Breath sounds vs. lung sounds: Are they synonymous or distinct terms in medical practice
- Types of Sounds: Crackles, wheezes, and stridor: How do they relate to breath and lung sounds
- Assessment Techniques: Stethoscope use: How are breath and lung sounds evaluated in clinical settings
- Pathological Differences: Do abnormal breath sounds always indicate lung issues, or are they separate entities
- Clinical Relevance: How do healthcare providers differentiate between breath and lung sounds in diagnosis
![]()
Definition Comparison: Breath sounds vs. lung sounds: Are they synonymous or distinct terms in medical practice?
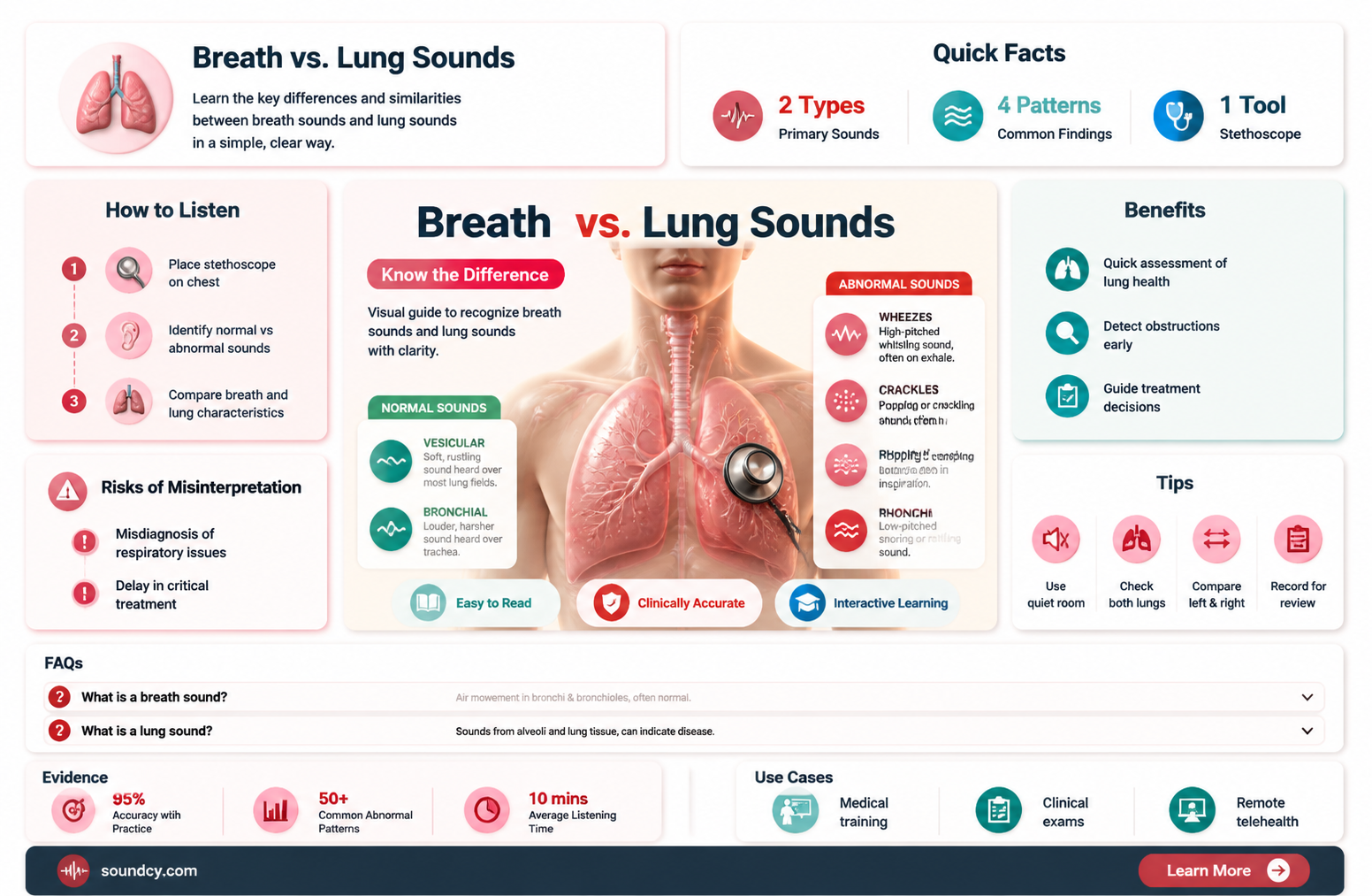
Breath sounds and lung sounds are terms often used interchangeably in medical discussions, yet their nuances reveal subtle distinctions. Breath sounds refer to the audible vibrations produced by air moving through the respiratory tract, encompassing the entire pathway from the nose or mouth to the alveoli. These sounds are categorized into normal (vesicular, bronchial) and abnormal (adventitious) types, each providing clues about respiratory health. Lung sounds, on the other hand, specifically denote the noises originating from the lungs themselves, often focusing on the alveoli and smaller airways. While both terms overlap significantly, the former is broader, while the latter is more localized.
To illustrate, consider auscultation during a physical exam. A clinician listens for vesicular breath sounds, which are soft and rustling, typically heard over most of the lung fields. If wheezing or crackles are detected, these are classified as adventitious breath sounds, indicating potential issues like asthma or pneumonia. In contrast, lung sounds in this context would specifically refer to the auditory cues emanating from the lung tissue itself, such as the intensity or quality of vesicular sounds over different lung regions. This distinction, though subtle, highlights the importance of precision in medical terminology.
From a practical standpoint, understanding the difference aids in accurate diagnosis and communication. For instance, a patient with chronic obstructive pulmonary disease (COPD) may exhibit prolonged expiratory phase breath sounds, while lung sounds might specifically describe the presence of rhonchi in the lower lobes. Misinterpreting these terms could lead to confusion in clinical notes or treatment plans. Thus, while breath sounds and lung sounds are closely related, their distinct scopes make them not entirely synonymous.
In medical practice, the choice of term often depends on context. For a general assessment, "breath sounds" suffices to describe the overall auditory findings. However, when pinpointing the origin of abnormal noises, "lung sounds" offers greater specificity. For example, a nurse documenting crackles heard over the lung bases would use "lung sounds" to emphasize the location. This clarity ensures that healthcare providers can collaborate effectively, tailoring interventions to the patient’s precise condition.
Ultimately, while breath sounds and lung sounds share considerable overlap, they are not identical. Breath sounds encompass the entire respiratory tract, whereas lung sounds focus on the lungs themselves. Recognizing this distinction enhances diagnostic accuracy and communication in clinical settings. Whether documenting findings or discussing a case, choosing the appropriate term ensures clarity and precision, which are paramount in medical practice.
Quick Guide: Activating Sound on Your QC35 Headphones Easily
You may want to see also
Explore related products






![]()
Types of Sounds: Crackles, wheezes, and stridor: How do they relate to breath and lung sounds?
Breath sounds and lung sounds are often used interchangeably, but they encompass a spectrum of auditory cues that reveal the health of the respiratory system. Among these, crackles, wheezes, and stridor stand out as distinct types, each pointing to specific underlying conditions. Crackles, for instance, are brief, discontinuous sounds resembling the crackling of paper and are typically heard during inhalation. They occur when air moves through airways filled with fluid, mucus, or secretions, commonly associated with conditions like pneumonia or heart failure. Wheezes, on the other hand, are high-pitched, continuous sounds caused by narrowed airways, often due to asthma, chronic obstructive pulmonary disease (COPD), or bronchitis. Stridor, a harsh, vibrating noise, is usually heard during inspiration and indicates a severe obstruction in the upper airway, such as from a foreign body or laryngeal edema.
To differentiate these sounds, consider their timing and characteristics. Crackles are often described as fine or coarse, with fine crackles being shorter and higher-pitched, heard in conditions like interstitial lung disease, while coarse crackles are louder and lower-pitched, associated with bronchiectasis or congestive heart failure. Wheezes can be monophonic (single-pitched) or polyphonic (multiple pitches), with the former suggesting a localized obstruction and the latter indicating widespread airway narrowing. Stridor is unique in its localization to the upper airway and is often an emergency, requiring immediate evaluation to rule out life-threatening causes like epiglottitis or anaphylaxis.
Clinicians rely on auscultation, the act of listening to internal sounds, to identify these abnormalities. A stethoscope is the primary tool, but advanced techniques like lung ultrasound or spirometry may be used for confirmation. For example, in pediatric patients, stridor in infants under 3 months often points to laryngomalacia, a condition where the cartilage of the larynx is soft, while in older children, it may indicate croup or a foreign body. In adults, wheezing accompanied by shortness of breath and chest tightness warrants a bronchodilator trial, with a 15-20% improvement in forced expiratory volume (FEV1) confirming reversible airway obstruction.
Understanding these sounds is crucial for timely intervention. Crackles may require diuretics in heart failure patients to reduce fluid overload, while wheezes often respond to inhaled corticosteroids or beta-agonists. Stridor demands urgent action, such as securing the airway or administering epinephrine in cases of anaphylaxis. Patients and caregivers can also benefit from recognizing these sounds, as early reporting can expedite diagnosis and treatment. For instance, a caregiver noticing stridor in a child should seek immediate medical attention, as delays can lead to respiratory distress.
In summary, crackles, wheezes, and stridor are distinct breath and lung sounds that provide critical insights into respiratory health. Their identification requires a keen ear, clinical knowledge, and sometimes advanced tools. By understanding their characteristics, causes, and implications, healthcare providers can tailor interventions effectively, improving patient outcomes. Whether in a hospital setting or at home, recognizing these sounds is a vital skill that bridges the gap between symptom and solution.
Are Sound Machines FSA Eligible? Exploring Sleep Aid Coverage Options
You may want to see also
Explore related products






![]()
Assessment Techniques: Stethoscope use: How are breath and lung sounds evaluated in clinical settings?
Breath sounds and lung sounds are often used interchangeably in clinical settings, but they encompass distinct auditory cues that provide critical insights into respiratory health. While breath sounds refer broadly to the noises produced during inhalation and exhalation, lung sounds specifically include both normal and abnormal auditory phenomena originating within the lungs. Clinicians use a stethoscope to auscultate these sounds, differentiating between healthy respiratory patterns and pathological conditions such as pneumonia, asthma, or chronic obstructive pulmonary disease (COPD). Mastery of this technique is essential for accurate diagnosis and timely intervention.
To evaluate breath and lung sounds effectively, begin by positioning the patient comfortably in a seated or supine position, ensuring relaxation to minimize artifactual noises. Use a stethoscope with a diaphragm for high-pitched sounds and a bell for low-pitched sounds, systematically auscultating all lung fields: anterior, posterior, and lateral. Normal breath sounds include vesicular (soft during inspiration, quieter during expiration) and bronchial (equal intensity during both phases). Abnormal sounds, such as wheezes, crackles, or stridor, indicate airway obstruction, fluid accumulation, or inflammation. For example, fine crackles heard in late inspiration suggest interstitial lung disease, while wheezes during expiration often point to asthma or COPD.
A structured approach enhances accuracy in auscultation. Divide the chest into six zones (upper, mid, and lower on both sides) and spend at least 5–10 seconds per zone, noting sound quality, intensity, and duration. Compare findings between corresponding lung fields to identify asymmetry, a key indicator of localized pathology. For pediatric patients, shorter auscultation times and age-specific sound expectations are necessary, as children’s respiratory rates are higher (e.g., 30–40 breaths/min in toddlers). In elderly patients, diminished sound intensity is common due to reduced lung elasticity, requiring careful differentiation from pathological conditions.
Caution must be exercised to avoid misinterpretation. Environmental factors like clothing friction or patient movement can mimic abnormal sounds. Always ensure the stethoscope diaphragm or bell is firmly placed on bare skin, and instruct the patient to breathe deeply and steadily. Document findings precisely, using standardized terminology (e.g., "bilateral wheezing in expiratory phase" or "fine crackles in left lower lobe"). This clarity aids in communication with colleagues and longitudinal monitoring of the patient’s condition.
In conclusion, stethoscope auscultation is a cornerstone of respiratory assessment, bridging the gap between breath and lung sounds to uncover underlying health issues. By combining technical precision with clinical acumen, healthcare providers can transform auditory cues into actionable insights, improving patient outcomes across diverse populations. Regular practice and adherence to best practices ensure proficiency in this vital skill.
Is a Pin Drop a Sound? Exploring the Science of Silence
You may want to see also
Explore related products






![]()
Pathological Differences: Do abnormal breath sounds always indicate lung issues, or are they separate entities?
Abnormal breath sounds often raise immediate concerns about lung health, but not all deviations from normal indicate pulmonary pathology. For instance, stridor—a high-pitched, musical sound—typically arises from upper airway obstruction, such as in croup or laryngeal edema, rather than lung tissue involvement. Similarly, gurgling or rattling sounds (known as rhonchi) can stem from excessive mucus in the throat or trachea, not necessarily the lungs. These examples highlight that while breath sounds are closely tied to lung function, they can also reflect issues in adjacent structures, underscoring the need for precise localization during auscultation.
To differentiate between lung-specific and extrathoracic abnormalities, clinicians must consider the sound’s characteristics and patient context. Wheezing, for example, is often associated with asthma or chronic obstructive pulmonary disease (COPD), but it can also occur in conditions like heart failure, where fluid accumulation in the lungs mimics bronchial constriction. Conversely, diminished breath sounds may suggest pneumothorax or consolidation in the lungs, but they can also result from poor patient effort or obstruction in the upper airways. A systematic approach—including history, physical exam, and imaging—is essential to avoid misattributing symptoms.
Instructively, auscultation should be paired with other diagnostic tools to confirm the origin of abnormal sounds. For instance, a chest X-ray or CT scan can identify lung parenchymal changes, while bronchoscopy may reveal airway tumors or foreign bodies causing stridor. In pediatric patients, particularly those under 5 years old, stridor often signals viral croup, a condition managed with humidified air and a single dose of dexamethasone (0.6 mg/kg), rather than lung-directed therapy. This underscores the importance of age-specific considerations in interpreting breath sounds.
Persuasively, it’s critical to recognize that abnormal breath sounds are not inherently diagnostic of lung disease but rather serve as clues in a broader clinical puzzle. For example, a patient with unilateral absent breath sounds could have a pneumothorax, but the same finding might indicate a tension pneumothorax requiring immediate needle decompression. Misinterpreting these sounds as benign could delay life-saving interventions. Thus, clinicians must remain vigilant, integrating auscultatory findings with other data to accurately pinpoint the source of pathology.
Comparatively, while breath sounds are often synonymous with lung sounds in practice, their interpretation requires a nuanced understanding of anatomy and physiology. For instance, crackles (formerly called rales) are traditionally linked to alveolar fluid in conditions like pneumonia or heart failure, but they can also occur in interstitial lung diseases like sarcoidosis. In contrast, pleural rubs—a creaking or grating sound—arise from inflamed pleural surfaces, not lung tissue itself. This distinction is vital, as treatments for pleurisy (e.g., NSAIDs) differ markedly from those for pulmonary edema (e.g., diuretics).
In conclusion, abnormal breath sounds are not exclusively indicators of lung issues but can reflect a spectrum of pathologies, from upper airway obstruction to pleural inflammation. Clinicians must approach auscultation with a critical eye, combining sound characteristics, patient history, and ancillary testing to accurately localize the source of abnormality. This precision ensures targeted treatment, avoiding the pitfalls of assuming breath sounds and lung sounds are always one and the same.
Choosing the Right Foam Thickness for Effective Sound Insulation
You may want to see also
Explore related products






![]()
Clinical Relevance: How do healthcare providers differentiate between breath and lung sounds in diagnosis?
Breath sounds and lung sounds, though often used interchangeably, are not synonymous in clinical practice. Breath sounds encompass the audible vibrations produced by air moving through the respiratory tract, including the nose, mouth, throat, and airways. Lung sounds, more specifically, refer to the auscultatory findings from the lungs themselves, such as vesicular breath sounds, crackles, wheezes, or stridor. This distinction is critical for healthcare providers, as misinterpreting these sounds can lead to diagnostic errors. For instance, wheezing heard over the throat is a breath sound, while wheezing localized to the lung fields is a lung sound, each pointing to different pathologies.
To differentiate between breath and lung sounds, clinicians follow a systematic approach during auscultation. First, they assess the location of the sound. Breath sounds originating from the upper airway, such as stridor or transmitted upper airway noises, are distinguished from those arising within the lung parenchyma. Second, they evaluate the characteristics of the sound. For example, crackles are typically lung sounds associated with conditions like pneumonia or heart failure, whereas stridor is a breath sound indicative of upper airway obstruction. Third, they consider the patient’s clinical context, including symptoms, medical history, and physical exam findings, to corroborate their interpretation.
Auscultation technique plays a pivotal role in this differentiation. Clinicians use a stethoscope to listen to specific lung fields, ensuring proper placement and patient positioning. For adults, the patient is typically seated or supine, while children may require more creative positioning to ensure cooperation. Providers listen for symmetry between lung fields, noting any deviations. For instance, asymmetrical wheezing may suggest localized bronchospasm, while bilateral crackles could indicate pulmonary edema. Proper technique minimizes artifacts, such as clothing rustling or stethoscope friction, which can mimic breath sounds.
Practical tips enhance accuracy in distinguishing these sounds. For example, asking the patient to take slow, deep breaths amplifies vesicular breath sounds, making them easier to assess. In pediatric patients, using a smaller stethoscope bell and warming the device can improve comfort and sound clarity. Clinicians should also be aware of age-related variations; children often exhibit louder breath sounds due to smaller airways, while elderly patients may have diminished lung sounds due to reduced air movement. These nuances guide providers in tailoring their diagnostic approach to individual patients.
Ultimately, the ability to differentiate between breath and lung sounds is a cornerstone of respiratory diagnosis. Misclassification can lead to inappropriate interventions, such as prescribing bronchodilators for upper airway stridor or overlooking pneumonia in the presence of crackles. By combining precise auscultation techniques, clinical context, and patient-specific considerations, healthcare providers can accurately interpret these sounds, ensuring targeted and effective care. Mastery of this skill not only improves diagnostic accuracy but also fosters trust in the clinician-patient relationship.
Understanding the Deep, Vibrant World of Bass Sound in Music
You may want to see also
Frequently asked questions
Yes, breath sounds and lung sounds are the same thing. They refer to the sounds produced by air moving through the respiratory tract during inhalation and exhalation.
They are called lung sounds because these sounds originate from the lungs and airways, reflecting the airflow and conditions within the respiratory system.
Yes, breath sounds can provide valuable information about lung health. Abnormal sounds, such as wheezing or crackles, may indicate conditions like asthma, pneumonia, or chronic obstructive pulmonary disease (COPD).
Yes, there are different types of breath sounds, including normal (vesicular) sounds, wheezes, crackles (rales), stridor, and ronchi, each associated with specific respiratory conditions.
Breath sounds are typically assessed using a stethoscope (auscultation) by a healthcare professional, who listens to different areas of the chest to evaluate lung function and detect abnormalities.