Adventitious breath sounds, also known as abnormal breath sounds, are additional noises detected during auscultation that deviate from the normal airflow patterns in the lungs. These sounds, such as wheezes, crackles, rhonchi, and stridor, can indicate underlying respiratory conditions or diseases. While normal breath sounds are typically characterized by quiet, smooth airflow, the presence of adventitious sounds often raises concerns about their significance and whether they are a cause for alarm. Understanding whether these sounds are normal or indicative of a pathological process is crucial for accurate diagnosis and appropriate management of respiratory health.
| Characteristics | Values |
|---|---|
| Definition | Abnormal lung sounds heard during auscultation, in addition to normal breath sounds. |
| Types | Crackles, wheezes, rhonchi, stridor, pleural friction rub. |
| Normalcy | Generally not normal; indicate underlying respiratory conditions. |
| Causes | Pneumonia, asthma, COPD, heart failure, pulmonary edema, foreign body aspiration, etc. |
| Crackles | Associated with fluid in alveoli (e.g., pneumonia, heart failure). |
| Wheezes | Linked to airway narrowing (e.g., asthma, COPD, bronchitis). |
| Rhonchi | Indicate mucus or fluid in larger airways (e.g., COPD, bronchitis). |
| Stridor | Suggests upper airway obstruction (e.g., croup, foreign body). |
| Pleural Friction Rub | Occurs with inflammation of the pleura (e.g., pleurisy). |
| Diagnosis | Requires medical evaluation, often with chest X-rays, CT scans, or pulmonary function tests. |
| Treatment | Depends on the underlying cause (e.g., antibiotics, bronchodilators, diuretics). |
| Prognosis | Varies based on the cause and timely intervention. |
Explore related products






What You'll Learn
![]()
Crackles and Wheezes: Understanding Adventitious Sounds
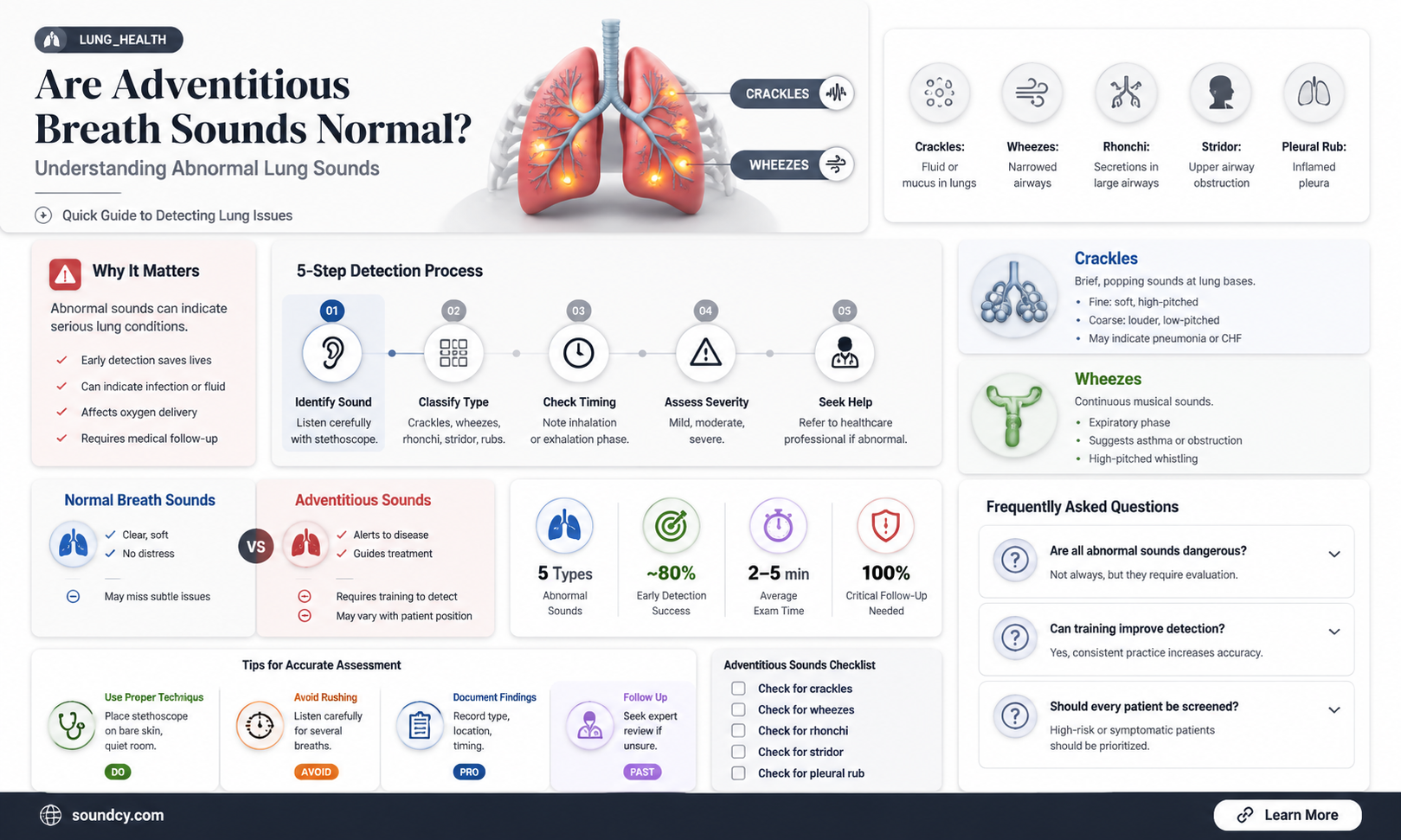
Adventitious breath sounds, such as crackles and wheezes, are abnormal lung sounds that can provide valuable insights into a patient's respiratory health. These sounds are not typically heard in normal breathing and often indicate underlying respiratory conditions. When auscultating a patient's lungs, healthcare providers listen for these sounds to diagnose and monitor various pulmonary disorders. Understanding the characteristics and implications of crackles and wheezes is essential for accurate assessment and patient care.
Crackles are one of the most common adventitious lung sounds, often described as brief, discontinuous, and popping noises. They are typically heard during inhalation and can be further classified into fine and coarse crackles based on their pitch and duration. Fine crackles are high-pitched and very brief, resembling the sound of opening a Velcro fastener, while coarse crackles are lower in pitch and slightly longer. These sounds are associated with the opening of small airways or alveoli that are filled with fluid, mucus, or other substances. Conditions such as pneumonia, heart failure, and interstitial lung diseases often present with crackles due to the accumulation of fluid in the lungs or inflammation of the alveolar walls.
Wheezes, on the other hand, are continuous musical sounds that occur due to the narrowing of airways. They are typically high-pitched and can be heard during both inhalation and exhalation, though they are often more prominent during exhalation. Wheezes result from the turbulent airflow through constricted or partially obstructed airways, commonly seen in asthma, chronic obstructive pulmonary disease (COPD), and bronchitis. The pitch and intensity of wheezes can vary depending on the severity of the airway obstruction. For instance, high-pitched wheezes may indicate severe bronchospasm, while low-pitched wheezes could suggest the presence of mucus or a foreign body in the larger airways.
It is important to note that while adventitious breath sounds like crackles and wheezes are not normal, their presence is not always indicative of a severe condition. The context, patient history, and other clinical findings play a crucial role in determining the significance of these sounds. For example, a few fine crackles at the lung bases in an elderly patient might be less concerning than widespread coarse crackles in a younger individual with a history of respiratory infections. Healthcare providers must consider the overall clinical picture to interpret these sounds accurately.
In clinical practice, recognizing and differentiating between crackles and wheezes is a fundamental skill for healthcare professionals. Proper auscultation techniques, combined with a thorough understanding of these sounds, enable early detection and management of respiratory issues. Patients experiencing persistent or worsening breath sounds should seek medical attention, as these could be symptoms of conditions requiring prompt treatment. By mastering the identification of adventitious breath sounds, medical practitioners can significantly improve patient outcomes and ensure timely interventions.
Mastering Sound Keys on Mac: A Step-by-Step Assignment Guide
You may want to see also
Explore related products






![]()
Causes of Abnormal Breath Sounds in Lungs
Abnormal breath sounds in the lungs, often referred to as adventitious breath sounds, are indicative of underlying respiratory conditions. These sounds, which include wheezes, crackles (rales), rhonchi, and stridor, are not normal and typically signal pathology. Understanding the causes of these abnormal sounds is crucial for accurate diagnosis and treatment. One common cause is chronic obstructive pulmonary disease (COPD), a progressive lung disease that obstructs airflow. Patients with COPD often exhibit wheezing, a high-pitched whistling sound caused by narrowed airways. This occurs due to inflammation and mucus buildup, which restrict air movement, particularly during exhalation.
Another significant cause of abnormal breath sounds is pneumonia, an infection that inflames the air sacs in one or both lungs. Crackles, which sound like popping or bubbling, are frequently heard in pneumonia patients. These sounds arise from fluid, mucus, or pus in the alveoli, which are normally air-filled. Crackles are particularly prominent during inhalation as air moves past the fluid-filled areas. Similarly, congestive heart failure (CHF) can lead to abnormal breath sounds, specifically crackles, due to pulmonary edema. In CHF, the heart’s inability to pump blood effectively causes fluid to accumulate in the lungs, resulting in crackles that are often worse when the patient is lying down.
Asthma is another condition that produces abnormal breath sounds, primarily wheezing. This occurs due to bronchoconstriction, where the muscles around the airways tighten, and inflammation causes swelling and mucus production. Wheezing in asthma is typically reversible with bronchodilators but can become persistent in severe or poorly managed cases. Additionally, bronchiectasis, a condition where the airways become permanently widened and scarred, often leads to rhonchi—a low-pitched rattling sound. This is caused by excessive mucus in the airways, which the patient may attempt to clear through coughing.
Foreign body aspiration or airway obstruction can also cause abnormal breath sounds, particularly stridor. Stridor is a high-pitched, musical sound that occurs during inspiration and is indicative of a partial obstruction in the upper airway, such as the trachea or larynx. This is often seen in children who have inhaled small objects but can also occur in adults due to tumors or swelling. Lastly, interstitial lung diseases (ILDs), such as pulmonary fibrosis, can produce fine or coarse crackles due to scarring and stiffening of lung tissue. These crackles are typically bilateral and persistent, reflecting the chronic nature of the disease.
In summary, abnormal breath sounds in the lungs are caused by a variety of conditions, each with distinct characteristics. Wheezing is commonly associated with COPD and asthma, crackles with pneumonia and CHF, rhonchi with bronchiectasis, and stridor with airway obstruction. Recognizing these sounds and their underlying causes is essential for healthcare providers to initiate appropriate diagnostic and therapeutic interventions. Adventitious breath sounds are not normal and always warrant further investigation to address the root cause of the respiratory issue.
Sound Rules: Movie Theaters and Their Regulations
You may want to see also
Explore related products






![]()
When Are Adventitious Sounds Considered Normal?
Adventitious breath sounds, also known as abnormal or added lung sounds, are often a cause for concern during respiratory assessments. However, it is essential to understand that not all adventitious sounds indicate a pathological condition. In certain situations, these sounds can be considered normal variants, especially when they are soft, few, and do not cause any symptoms. So, when are adventitious breath sounds deemed normal?
Physiological Variations: In healthy individuals, particularly children and young adults, occasional adventitious sounds may be heard without any underlying disease. Fine crackles, for instance, can be a normal finding in children and are often referred to as 'physiological crackles.' These sounds are typically soft and can be heard at the end of inspiration, especially during deep breathing. Similarly, some people may exhibit soft wheezes during forced expiration, which can be a normal variant, especially in those with a history of allergies or asthma, as long as it is not associated with respiratory distress.
Post-Exertion and Environmental Factors: After strenuous exercise or physical activity, it is not uncommon to detect adventitious breath sounds. This is particularly true for crackles, which may be heard in healthy individuals post-exercise due to increased blood flow and fluid movement in the lungs. Additionally, environmental factors can play a role. For example, breathing in cold air can lead to the production of crackles, especially in healthy young adults, and this is usually a temporary and harmless phenomenon.
Asymptomatic Individuals: In the absence of respiratory symptoms, certain adventitious sounds might be considered normal. For instance, fine crackles heard in the lung bases of an asymptomatic person during a routine check-up may not necessarily indicate a problem. However, this requires careful clinical judgment, as the presence of multiple types of adventitious sounds or their occurrence in specific lung regions could still suggest an underlying issue.
It is crucial to emphasize that the context and associated symptoms play a significant role in determining the significance of adventitious breath sounds. While some situations allow for these sounds to be considered normal, any persistent or concerning symptoms, such as cough, shortness of breath, or chest pain, warrant further investigation. Healthcare professionals should always consider the patient's medical history, perform a comprehensive physical examination, and, if necessary, order additional tests to differentiate between normal variants and pathological conditions. Understanding when adventitious breath sounds are typical is essential for accurate diagnosis and patient reassurance.
Mastering Raspberry Pi Sound Writing: A Comprehensive Guide for Beginners
You may want to see also
Explore related products






![]()
Diagnosing Lung Conditions via Breath Sounds
Diagnosing lung conditions often begins with a simple yet powerful tool: listening to breath sounds. Auscultation, the act of listening to the internal sounds of the body, allows healthcare professionals to detect abnormalities in lung function. Normal breath sounds are typically quiet and consistent, consisting of vesicular breathing during inspiration and expiration. However, the presence of adventitious breath sounds—abnormal sounds that are added to normal breathing—can indicate underlying lung conditions. These sounds are not normal and often serve as critical indicators of respiratory pathology. Understanding and interpreting these sounds is essential for accurate diagnosis and timely intervention.
Adventitious breath sounds can be categorized into continuous and discontinuous types. Continuous sounds, such as wheezes and rhonchi, are typically associated with airway obstruction. Wheezes, high-pitched whistling sounds, are commonly heard in conditions like asthma or chronic obstructive pulmonary disease (COPD), where narrowed airways restrict airflow. Rhonchi, on the other hand, are low-pitched, snoring-like sounds often caused by mucus or secretions in larger airways, as seen in chronic bronchitis. Discontinuous sounds, like crackles (also known as rales) and stridor, provide additional diagnostic clues. Crackles are brief, popping sounds that occur during inspiration and are often linked to fluid accumulation in the alveoli, as seen in pneumonia or heart failure. Stridor, a high-pitched, musical sound heard during inspiration, suggests severe upper airway obstruction, such as in croup or a foreign body aspiration.
The timing and characteristics of adventitious breath sounds are crucial for diagnosis. For instance, crackles that are heard at the beginning of inspiration suggest conditions like interstitial lung disease, while those heard throughout inspiration may indicate fluid overload. Wheezes that are present during both inspiration and expiration often signify severe airway obstruction. Healthcare providers use this information, combined with patient history and physical examination findings, to narrow down potential diagnoses. For example, a patient with a history of smoking, chronic cough, and bilateral wheezes is likely suffering from COPD, while a child with stridor and a recent upper respiratory infection may have croup.
Advanced techniques, such as using electronic stethoscopes or recording breath sounds for analysis, can enhance diagnostic accuracy. These tools allow for amplification and visualization of sounds, making subtle abnormalities easier to detect. Additionally, integrating auscultation with other diagnostic modalities, such as chest X-rays, CT scans, and pulmonary function tests, provides a comprehensive understanding of the patient’s condition. Early recognition of adventitious breath sounds can lead to prompt treatment, preventing disease progression and improving patient outcomes.
In conclusion, adventitious breath sounds are not normal and serve as vital clues in diagnosing lung conditions. By carefully listening to and interpreting these sounds, healthcare professionals can identify underlying pathologies, from asthma and pneumonia to COPD and heart failure. Mastery of auscultation techniques, combined with clinical judgment and advanced tools, ensures accurate diagnosis and effective management of respiratory disorders. Recognizing the significance of these abnormal sounds is a cornerstone of respiratory care, emphasizing the importance of this fundamental skill in medical practice.
The Most Unbearable Noises and How They Affect Us
You may want to see also
![]()
Treatment Options for Abnormal Respiratory Noises
Adventitious breath sounds, also known as abnormal respiratory noises, are additional sounds heard during auscultation that are not part of normal breathing. These sounds, such as wheezes, crackles, rhonchi, and stridor, often indicate underlying respiratory conditions. While they are not normal, their treatment depends on the specific cause and severity of the condition. Identifying the root cause is crucial for effective management, as these sounds can stem from issues like asthma, chronic obstructive pulmonary disease (COPD), pneumonia, or heart failure.
Pharmacological Interventions are a cornerstone in treating abnormal respiratory noises. For example, bronchodilators like albuterol are commonly prescribed for wheezing associated with asthma or COPD, as they relax the airway muscles and improve airflow. Inhaled corticosteroids may also be used to reduce inflammation in chronic conditions. For crackles caused by fluid accumulation in the lungs, diuretics can help manage heart failure or pulmonary edema by reducing excess fluid. Antibiotics are essential for treating infectious causes, such as pneumonia or bronchitis, which often produce crackles or rhonchi.
Non-Pharmacological Treatments play a significant role in managing abnormal breath sounds. Pulmonary rehabilitation programs, including breathing exercises and physical therapy, can improve lung function and reduce symptoms like wheezing or stridor. Chest physiotherapy, such as postural drainage and percussion, helps clear mucus from the airways, alleviating rhonchi or crackles in conditions like cystic fibrosis or bronchiectasis. For stridor caused by upper airway obstruction, techniques like airway clearance devices or positional changes can provide relief.
Oxygen Therapy is often necessary for patients with severe respiratory distress or hypoxemia, which may accompany abnormal breath sounds. Supplemental oxygen can be delivered via nasal cannula, mask, or in severe cases, through non-invasive ventilation (NIV) or mechanical ventilation. This treatment ensures adequate oxygenation while the underlying cause is addressed.
Surgical and Invasive Procedures may be required for certain conditions causing abnormal respiratory noises. For example, stridor due to tracheal stenosis or vocal cord paralysis may necessitate surgical intervention to widen the airway or correct the obstruction. In cases of severe COPD or cystic fibrosis, lung transplantation may be considered as a last resort. Bronchoscopy can also be used diagnostically and therapeutically to remove foreign bodies or clear airway obstructions causing abnormal sounds.
Lifestyle and Preventive Measures are essential in managing and preventing abnormal breath sounds. Smoking cessation is critical for patients with COPD or chronic bronchitis, as it reduces airway inflammation and mucus production. Avoiding environmental triggers, such as allergens or pollutants, can prevent exacerbations of asthma or other respiratory conditions. Regular vaccinations, including the flu and pneumonia vaccines, are recommended to reduce the risk of infections that may cause adventitious sounds.
In conclusion, treatment options for abnormal respiratory noises are diverse and tailored to the underlying cause. A combination of pharmacological, non-pharmacological, and invasive approaches may be necessary to manage symptoms effectively. Early diagnosis and intervention are key to improving outcomes and quality of life for patients experiencing these abnormal breath sounds.
Emphysema: Clear Lung Sounds or a Myth?
You may want to see also
Frequently asked questions
No, adventitious breath sounds are not always abnormal. Some, like mild crackles or wheezes, can occur temporarily due to factors like exercise, cold air, or minor respiratory irritation. However, persistent or severe adventitious sounds often indicate an underlying condition.
Yes, children can sometimes have transient adventitious breath sounds, especially during respiratory infections or after crying. However, persistent or recurrent sounds should be evaluated by a healthcare provider to rule out conditions like asthma or pneumonia.
Yes, it is common to hear adventitious breath sounds, such as crackles or wheezes, during or after a cold or flu due to mucus buildup or airway inflammation. These sounds typically resolve as the illness clears, but prolonged symptoms warrant medical attention.